
Клинический разбор в общей медицине №04 2026
GLP-1 Receptor Agonists in Nonalcoholic Fatty Pancreas Disease: Evidence, Mechanisms, and Future Directions
Номера страниц в выпуске:60-65
Abstract
Pancreatic steatosis (fatty pancreas) has emerged as a key pathological condition associated with metabolic dysfunction, impaired β-cell function, exocrine insufficiency, and an increased risk of pancreatitis and pancreatic cancer.
Aim. This review synthesizes current preclinical and clinical evidence on the effects of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) on pancreatic fat, elucidates the underlying mechanisms, discusses safety concerns, and highlights research gaps.
Materials and methods. A narrative literature review was performed using PubMed and Scopus (2010–2025) with the keywords “GLP-1 receptor agonists,” “fatty pancreas,” and “nonalcoholic fatty pancreas disease (NAFPD)”, including both experimental and clinical investigations.
Results. GLP-1 RAs – including liraglutide, semaglutide, dulaglutide, and emerging dual agonists – exert potent metabolic benefits by reducing body weight, visceral adiposity, and hepatic steatosis. Recent MRI-based studies employing proton density fat fraction quantification indicate that GLP-1 RAs can reduce intrapancreatic fat by up to 20–30% after 24 weeks of therapy. These findings suggest a potentially direct role in ameliorating pancreatic steatosis beyond global weight loss effects.
Conclusion. GLP-1 RAs represent a promising therapeutic strategy for mitigating pancreatic steatosis and its systemic metabolic consequences. Nevertheless, clinical evidence remains limited, and the mechanisms underlying pancreatic fat reduction – whether weight-dependent or independent – require further elucidation. Longitudinal, imaging-based randomized controlled trials are urgently needed to establish causality and clarify the full therapeutic potential of GLP-1 RAs in nonalcoholic fatty pancreas disease.
Keywords: pancreatic steatosis, nonalcoholic fatty pancreas disease (NAFPD), GLP-1 receptor agonists, liraglutide, semaglutide, intrapancreatic fat.
For citation: Abdelmoaty A.A., Alsadik M.A., Abdel-Sater Kh.A. GLP-1 Receptor Agonists in Nonalcoholic Fatty Pancreas Disease: Evidence, Mechanisms, and Future Directions. Clinical review for general practice. 2026; 7 (2): 60–65. DOI: 10.47407/kr2026.7.4.00822
Pancreatic steatosis (fatty pancreas) has emerged as a key pathological condition associated with metabolic dysfunction, impaired β-cell function, exocrine insufficiency, and an increased risk of pancreatitis and pancreatic cancer.
Aim. This review synthesizes current preclinical and clinical evidence on the effects of glucagon-like peptide-1 receptor agonists (GLP-1 RAs) on pancreatic fat, elucidates the underlying mechanisms, discusses safety concerns, and highlights research gaps.
Materials and methods. A narrative literature review was performed using PubMed and Scopus (2010–2025) with the keywords “GLP-1 receptor agonists,” “fatty pancreas,” and “nonalcoholic fatty pancreas disease (NAFPD)”, including both experimental and clinical investigations.
Results. GLP-1 RAs – including liraglutide, semaglutide, dulaglutide, and emerging dual agonists – exert potent metabolic benefits by reducing body weight, visceral adiposity, and hepatic steatosis. Recent MRI-based studies employing proton density fat fraction quantification indicate that GLP-1 RAs can reduce intrapancreatic fat by up to 20–30% after 24 weeks of therapy. These findings suggest a potentially direct role in ameliorating pancreatic steatosis beyond global weight loss effects.
Conclusion. GLP-1 RAs represent a promising therapeutic strategy for mitigating pancreatic steatosis and its systemic metabolic consequences. Nevertheless, clinical evidence remains limited, and the mechanisms underlying pancreatic fat reduction – whether weight-dependent or independent – require further elucidation. Longitudinal, imaging-based randomized controlled trials are urgently needed to establish causality and clarify the full therapeutic potential of GLP-1 RAs in nonalcoholic fatty pancreas disease.
Keywords: pancreatic steatosis, nonalcoholic fatty pancreas disease (NAFPD), GLP-1 receptor agonists, liraglutide, semaglutide, intrapancreatic fat.
For citation: Abdelmoaty A.A., Alsadik M.A., Abdel-Sater Kh.A. GLP-1 Receptor Agonists in Nonalcoholic Fatty Pancreas Disease: Evidence, Mechanisms, and Future Directions. Clinical review for general practice. 2026; 7 (2): 60–65. DOI: 10.47407/kr2026.7.4.00822
Агонисты рецепторов ГПП-1 при неалкогольной жировой болезни поджелудочной железы: факты, механизмы и направления дальнейших исследований
Ахмед A. Абдельмуати, Маха Е. Альсадик, Халед А. Абдель-СатерУниверситет Мута, Эль-Карак, Иордания
Kabdelsater@mutah.edu.jo
Аннотация
Стеатоз (липоматоз) поджелудочной железы стал основным патологическим состоянием, связанным с нарушениями обмена веществ, нарушением функции β-клеток, экзокринной недостаточностью, а также с повышением риска развития панкреатита и рака поджелудочной железы.
Цель. В настоящем обзоре обобщены имеющиеся данные доклинических и клинических исследований о действии агонистов рецепторов глюкагоноподобного пептида-1 (АР ГПП-1) на накапливающийся в поджелудочной железе жир, разъяснены механизмы их действия, представлено обсуждение вопросов безопасности, отмечены пробелы в исследованиях.
Материалы и методы. Выполнен обзор литературы с использованием баз данных PubMed и Scopus (2010–2025). Использованы ключевые слова «агонисты рецепторов ГПП-1», «стеатоз поджелудочной железы» и «неалкогольная жировая болезнь поджелудочной железы (НАЖБПЖ)». В обзор включены как экспериментальные, так и клинические исследования.
Результаты. АР ГПП-1, включая лираглутид, семаглутид, дулаглутид и недавно появившиеся двойные агонисты, оказывают мощное воздействие на обмен веществ, снижая массу тела, уменьшая висцеральное ожирение и стеатоз печени. Недавние исследования с применением магнитно-резонансной томографии, предполагавшие количественную оценку протонной плотности жировой фракции, показали, что АР ГПП-1 способны уменьшить количество накопившегося в поджелудочной железе жира на 20–30% после 24 нед терапии. Такие результаты указывают на возможное непосредственное участие в уменьшении стеатоза поджелудочной железы, выходящее за рамки общего эффекта снижения массы тела.
Заключение. Применение АР ГПП-1 представляет собой перспективную терапевтическую стратегию уменьшения стеатоза поджелудочной железы и смягчения его системного воздействия на обмен веществ. Тем не менее клинических данных все еще недостаточно. Необходимы дальнейшие исследования механизмов, лежащих в основе уменьшения количества накопившегося в поджелудочной железе жира, на предмет того, зависят они от массы тела или нет. Для установления причинно-следственной связи и окончательного выяснения терапевтического потенциала АР ГПП-1 при неалкогольной жировой болезни поджелудочной железы срочно необходимы продольные рандомизированные контролируемые исследования с применением методов медицинской визуализации.
Ключевые слова: стеатоз поджелудочной железы, неалкогольная жировая болезнь поджелудочной железы (НАЖБПЖ), агонисты рецепторов ГПП-1, лираглутид, семаглутид, накопление жира в поджелудочной железе.
Для цитирования: Абдельмуати А.А., Альсадик М.Е., Абдель-Сатер Х.А. Агонисты рецепторов ГПП-1 при неалкогольной жировой болезни поджелудочной железы: факты, механизмы и направления дальнейших исследовани. Клинический разбор в общей медицине. 2026; 7 (4): 60–65. DOI: 10.47407/kr2026.7.4.00822
Introduction
Pancreatic steatosis is defined as the ectopic accumulation of fat in the pancreas. Historically, pancreatic fat was regarded as an incidental finding. However, recent evidence shows it is a modifiable risk factor for diabetes and pancreatic malignancy [1].
The accumulation of fat in the pancreas is referred to by several synonyms, including fatty pancreas, pancreatic lipomatosis, and pancreatic lipidosis. Lipomatous pseudohypertrophy represents an extreme variant of pancreatic fat accumulation, characterized by pancreatic enlargement and replacement of the exocrine system by fat, with no association with obesity [2]. Pancreatic steatosis mainly involves the interlobular and intralobular spaces, usually sparing the intra-acinar space, where the exocrine cells reside, and the endocrine cells [3, 4].
By contrast, in metabolic dysfunction-associated steatotic liver disease, lipid accumulation predominately occurs intracellularly within hepatocytes [5]. Nonalcoholic Fatty Pancreas Disease (NAFPD) refers to fat accumulation related to obesity and/or metabolic syndrome in the absence of significant alcohol intake. Whether the nomenclature for NAFPD should be updated to Metabolic Dysfunction-Associated Steatotic Pancreas Disease, in line with the recent shift from Nonalcoholic Fatty Liver Disease to Metabolic Dysfunction-Associated Steatotic Liver Disease, remains an open question [6].
Pancreatic fat accumulation increases with age, and replacement of more than 25% of the pancreas by fat is associated with severe generalized atherosclerosis and increased risk of development of diabetes mellitus type 2 [7]. Pancreatic steatosis is the most commonly identified pancreatic pathology during radiological examination. Improved imaging techniques (MRI proton density fat fraction, quantitative computed tomography (CT) measures) have made detection and quantification more feasible.
The clinical significance of NAFPD cannot be overstated. The presence of ectopic fat in the pancreas is strongly linked to impaired insulin secretion, chronic inflammation, and a heightened risk for serious pancreatic pathologies, including pancreatitis and pancreatic cancer. Given the global rise in obesity and metabolic syndrome, NAFPD is becoming a major public health concern. This review aims to explore the therapeutic potential of GLP-1 RAs, a class of drugs with proven metabolic benefits, as a novel strategy for managing NAFPD.
Epidemiology and Clinical Significance
Prevalence estimates of pancreatic steatosis vary depending on the population and imaging modality; studies report rates from 10% to over 50% in at-risk groups (obesity, diabetes mellitus type 2). Observational studies have linked higher intrapancreatic fat with impaired insulin secretion, increased markers of inflammation, and a potential association with pancreatitis and pancreatic neoplasia, though causality remains unclear [8, 9]. Prevalence appears higher in East Asian and Mediterranean cohorts, mirroring obesity and metabolic trends [9].
Pathogenetic Mechanisms and Clinical Entities Associated with NAFPD (see Figure)
The main risk factors associated with NAFPD are obesity and metabolic syndrome (including dyslipidemia), while alcohol, viruses, iron deposition, drugs, and pancreatic duct obstruction represent potential secondary hits which participate in cell death and replacement of pancreatic tissue with fat [10–13].The main pathogenic mechanism of NAFPD is fatty replacement, followed by fatty accumulation (intra- or inter-lobular) and, ultimately, β-cell dysfunction [14]. Mechanisms associated with fat accumulation include:
Oxidative Stress: excessive accumulation of free fatty acids (FFAs) promotes mitochondrial dysfunction and reactive oxygen species generation, leading to lipid peroxidation and β-cell injury [15].
Inflammation: proinflammatory cytokines such as [Tumor necrosis factorα (TNFα), Interleukin-1 beta (IL-1β), Interleukin-6 (IL-6), monocyte chemoattractant protein-1] are upregulated, contributing to local inflammation and pancreatic stellate cell activation [16].
Hormonal Imbalance: alterations in adipokines – particularly decreased adiponectin and increased leptin and ghrelin – exacerbate lipid accumulation and impair insulin signaling [15, 16].
Stellate Cell Activation: activated pancreatic stellate cells drive fibrosis and perpetuate chronic inflammation, linking NAFPD to pancreatitis and neoplasia [17].
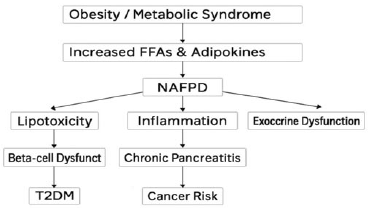
Proposed mechanisms linking obesity and metabolic dysfunction to NAFPD. The diagram illustrates the progression from obesity and elevated free fatty acids to NAFPD, leading to lipotoxicity, inflammation, β-cell dysfunction, and increased risks of diabetes and cancer.
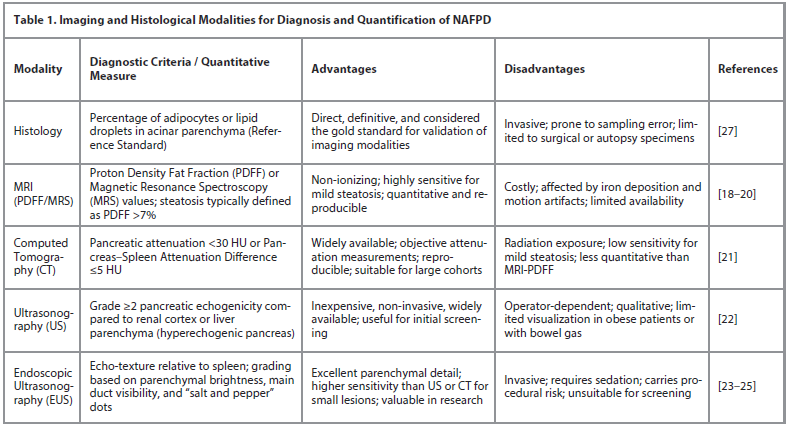
Diagnostic Methods and Quantification
The accurate diagnosis and quantification of pancreatic fat are crucial for both clinical management and research. The following Table 1 summarizes the main imaging modalities used for NAFPD assessment.
Magnetic Resonance Imaging (MRI)
MRI is currently the most accurate noninvasive modality. Techniques include: chemical shift imaging (Dixon method), MRI proton density fat fraction (MRI-PDFF), and Magnetic Resonance Spectroscopy (MRS) [18, 19]. PDFF values reported in healthy pancreas average 2–6%, while steatosis is often defined above 7% in research cohorts [20]. Non-ionization, reproducibility, and sensitivity to mild fat accumulation are advantages of MRI, while costliness, motion artifacts, and affection by iron deposition are considered limitations of its use [21].
Computed Tomography (CT)
CT is widely available and provides objective attenuation measurements. It depends on fat decreases tissue attenuation. Common thresholds for fatty pancreas: pancreas Hounsfield units <30 or pancreas–spleen attenuation difference ≤5 Hounsfield units [21]. Accessibility and reproducibility are advantages of CT, while radiation exposure and low sensitivity for mild steatosis are considered limitations of its use.
Ultrasonography and Endoscopic
Ultrasonography (EUS)
Ultrasonography is widely available to detect pancreatic steatosis, but obesity and bowel gas may cause invisibility of the pancreas. To diagnose pancreatic steatosis, pancreas echogenicity is traditionally compared with kidney echogenicity. Hyperechogenic pancreas can be seen in both pancreatic fibrosis and in fatty pancreas. Pancreatic steatosis can be classified into four grades by identifying patterns of pancreas echogenicity in abdominal Ultrasonography [22].
Diagnostic accuracy of pancreatic steatosis by endoscopic ultrasound (EUS) is superior to CT scan and magnetic resonance imaging (MRI). The disadvantages include its invasive nature, the risk of complications, and the need for sedation. EUS is considered a highly sensitive investigation for pancreatic examination, but till now pancreatic biopsy is the best method to measure pancreatic fat concentration [23]. However, it is unethical to use EUS as a screening tool [24]. EUS grading system adapted from radiology incorporating the echo-texture of the pancreas relative to the spleen as well as the ability to visualize the main pancreatic duct and “salt and pepper” dots in the parenchyma has been suggested to assess fatty pancreas [25].
Emerging Techniques
Elastography and Controlled Attenuation Parameter (CAP): proven in liver but still experimental for pancreas [26].
Histology: The Reference Standard
Histological assessment provides direct visualization of fat infiltration and remains the reference standard. Quantification is typically expressed as the percentage of adipocytes/lipid droplets in acinar parenchyma. However, it is invasive and prone to sampling error due to heterogeneous fat distribution. Hence, histology is primarily used for validation of imaging modalities [27].
Mechanisms of Action of GLP-1 Receptor
Agonists in Fatty Pancreas
GLP-1 RAs exert their beneficial effects on the fatty pancreas by combining systemic metabolic improvements with direct organ-specific actions. The clinical relevance of these mechanisms is increasingly being explored:
a. Improved Glycemic Control and Reduced Hyperinsulinemia. GLP-1 RAs enhance glucose-dependent insulin secretion and suppress inappropriate glucagon release, leading to improved glycemic control. Chronic hyperglycemia and hyperinsulinemia is thereby reduced by GLP-1 RAs, attenuating lipogenesis and lessening lipotoxic stress in pancreatic tissue [28].
b. Weight Loss and Reduction of Free Fatty Acid Efflux. GLP-1 RAs promote satiety, reduce food intake, and delay gastric emptying; this results in significant weight loss. The reduction in visceral adiposity decreases the free fatty acid flux into the pancreas, thereby decreasing pancreatic triglyceride accumulation [29, 30].
c. Direct Reduction of Intrapancreatic Fat. Clinical imaging studies indicate that GLP-1 RAs, particularly liraglutide, may reduce pancreatic triglyceride content. These effects are partially weight-dependent, but some evidence suggests weight- independent mechanisms [30]. For instance, the observed reduction in pancreatic fat fraction via MRI-PDFF in human trials, even after adjusting for weight loss, strongly supports a direct or preferential effect on pancreatic lipid metabolism.
d. Anti-inflammatory Effects. Pancreatic steatosis is characterized by the presence of local inflammation. GLP-1 RAs downregulate pro-inflammatory cytokines, for example, TNF-α and IL-6, while inhibiting NF-κB (Nuclear factor kappa-light-chain-enhancer of activated B cells) signaling and promoting anti-inflammatory pathways, which decrease pancreatic inflammation and prevent disease progression [31]. Preclinical data on a reduction in pancreatic NF-κB signaling in parallel with improved MRI fat fraction in human studies links the anti-inflammatory mechanism to the clinical outcome of fat reduction.
e. Reduction of Oxidative and Endoplasmic Reticulum Stress. Lipotoxicity in the pancreas is mediated through oxidative stress and endoplasmic reticulum dysfunction; GLP-1 RAs improve cellular stress responses by enhancing antioxidant defenses, alleviating endoplasmic reticulumc stress, and protecting pancreatic β-cells and acinar cells from apoptosis [28].
f. Direct Effects on Pancreatic Cells. GLP-1 receptors are expressed both in the islet β-cells and acinar tissue. Receptor activation promotes β-cell proliferation, survival, and insulin secretion, while modulating intracellular lipid metabolism through different pathways [28].
g. Weight-Independent Mechanisms. Indeed, there is emerging evidence that GLP-1 RAs may modulate the transcriptional regulators of lipid metabolism, including upregulation of fatty acid oxidation and downregulation of lipogenesis, independent of body weight reduction. These effects, though less well established, provide a potential direct mechanism of action [30].
Collectively, these mechanisms suggest that GLP-1 receptor agonists ameliorate NAFPD through both systemic and local effects. Systemically, they reduce caloric intake, visceral adiposity, and circulating FFAs, thereby limiting lipid oversupply to the pancreas. Locally, they attenuate inflammation, oxidative stress, and stellate cell activation, and improve β-cell survival. These convergent actions position GLP-1 RAs as dual modulators of metabolic and pancreatic health.
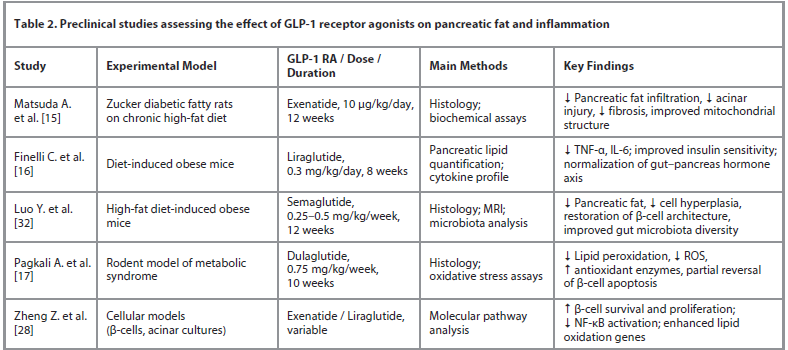
Preclinical Evidence for Pancreatic Fat Reduction
Animal studies consistently demonstrate that GLP-1 RAs reduce ectopic fat deposition and inflammatory signaling within the pancreas. For example, semaglutide and liraglutide in obese rodent models lower pancreatic triglyceride accumulation, normalize mitochondrial morphology, and reduce NF-κB activation [32]. However, most preclinical work remains short-term and lacks histologic quantification. Table 2 summarizes key preclinical studies examining pancreatic fat modulation by GLP-1 RAs.
Clinical Evidence for Pancreatic Fat Reduction
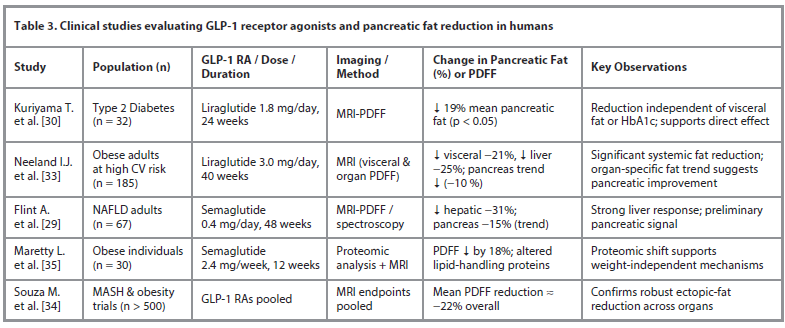
Emerging clinical evidence demonstrates that GLP-1 receptor agonists can reduce pancreatic fat content across diverse populations and study designs (Table 3), with effects that may extend beyond weight loss and glycemic control. Direct clinical evidence remains limited but emerging. Important studies include:
a. Kuriyama T. et al. [30]. In this prospective study, intrapancreatic fat was measured by MRI techniques. The study reported a statistically significant reduction in intrapancreatic fat following liraglutide treatment (duration and dose per study protocol). The reduction seemed to be independent of changes in HbA1c and visceral fat volume, suggesting a possible direct or preferential effect on pancreatic ectopic fat.
Critical Discussion of Kuriyama T. et al. Although this thus far represents the best preliminary evidence, interpretation of these results should be guarded because of several deficiencies in the study design. The sample size was small and the duration of follow-up fairly short. The open-label, single-arm design does not allow for a placebo or active comparator group, and thus it cannot be concluded with certainty that the observed fat reduction is due to the liraglutide treatment rather than other potential confounding factors or natural history. Future randomized controlled trials are essential to confirm these encouraging initial findings.
b. Indirect Evidence. Larger phase 2–3 trials of semaglutide and liraglutide show marked reductions in hepatic fat and visceral adipose tissue over 24–72 weeks. Given systemic effects on fat distribution, it is plausible that pancreas fat may also decline with longer durations and higher potency agents [33, 34].
c. Organ-Specific Mechanisms. There are suggestions that intrapancreatic fat reduction can occur independently of visceral fat loss, implying certain organ-specific mechanisms, including improved local lipolysis, changes in pancreatic blood flow, or direct receptor-mediated effects. Following semaglutide treatment, proteomic analyses show changes in proteins associated with pancreatic endocrine and exocrine function, as well as in adipogenesis and lipid metabolism [35].
Safety Considerations
GLP-1 receptor agonists (GLP-1 RAs) provide substantial metabolic and hepatic benefits, but pancreatic safety remains a critical consideration. Specific concerns have included reports of pancreatitis and the theoretical risk of pancreatic hyperplasia. Large observational studies and meta-analyses offer largely reassuring evidence: no significant increase in acute pancreatitis has been observed compared with other antidiabetic therapies [36–45], although some analyses suggested a small but statistically significant association (early reports [40–43]). Similarly, long-term studies show no increased risk of pancreatic cancer with GLP-1 RA use [36], with earlier signals likely confounded by study limitations. Mild, transient elevations in amylase or lipase may occur [41] but are not predictive of pancreatitis, and routine testing is unnecessary unless patients develop symptoms. Overall, the absolute risk appears low, but increased vigilance is warranted in patients with prior pancreatitis, gallstones, or hypertriglyceridemia. Long-term surveillance through registries is recommended to track pancreatic endpoints – including pancreatitis recurrence, neoplastic changes, imaging outcomes, and enzyme kinetics – to further clarify the safety profile of chronic GLP-1 RA therapy [45].
Critical Gaps and Recommended Study Designs
a. Studies specifically designed as RCTs that incorporate intrapancreatic fat measurement by MRI-PDFF or MRS both before and after GLP-1 RA therapy with appropriate sample sizes and follow-up of 6–24 months.
b. Multiple phenotypes will be included: obesity without diabetes, prediabetes, diabetes mellitus type 2, and post-pancreatitis patients.
c. Correlative Outcomes: changes in β-cell function represented by glucose-stimulated insulin secretion, exocrine markers, pancreatic enzyme levels, and clinical outcomes including pancreatitis, glycemic control.
d. Dose-response studies comparing agents, like liraglutide versus semaglutide and tirzepatide, and higher doses, for example, semaglutide 2.4 mg versus emerging higher doses.
e. Long-term safety registries with a focus on pancreatic outcomes and cancer surveillance.
Practical Clinical Implications
Clinicians may reasonably consider GLP-1 receptor agonists for obese or diabetic patients with imaging-confirmed NAFPD, given their systemic benefits and potential to reduce pancreatic fat. However, routine pancreatic imaging for all patients is not yet recommended outside research protocols. Close monitoring for abdominal pain or enzyme elevation remains advisable.
Conclusion
GLP-1 receptor agonists have great promise in improving systemic metabolic health and reducing hepatic steatosis and visceral adiposity, and may also reduce intrapancreatic fat.
Key Findings. A growing body of evidence, especially from advanced imaging studies, has suggested that this class of drugs could significantly reduce pancreatic fat content – a novel therapeutic approach in the management of NAFPD.
Research Priorities. There is still an urgent need for randomised controlled trials of adequate sample size and longer follow-up to confirm these findings and clarify the precise mechanisms, whether weight-dependent or independent, by which these drugs operate.
Final Message. Given that the prevalence of NAFPD is increasing and affects metabolic and pancreatic health, defining the full role of GLP-1 RAs in the management of pancreatic fat represents a top research priority and promises to open up new avenues to improve clinical outcomes among at-risk patients.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Ahmed A Abdelmoaty – Assoc. Prof., Department of Internal and Forensic Medicine, Faculty of Medicine, Mutah University. E-mail: drahmedatya33@mutah.edu.jo; ORCID: 0000-0002-3639-1803
Ахмед A. Абдельмуати – доц. каф. внутренних болезней и судебной медицины лечебного фак-та Университета Мута. E-mail: drahmedatya33@mutah.edu.jo; ORCID: 0000-0002-3639-1803
Maha E. Alsadik – Assoc. Prof., Department of Internal and Forensic Medicine, Faculty of Medicine, Mutah University. E-mail: mahaalsadik@mutah.edu.jo; ORCID: 0000-0002-4895-5936
Маха Е. Альсадик – доц. каф. внутренних болезней и судебной медицины лечебного фак-та Университета Мута. E-mail: mahaalsadik@mutah.edu.jo; ORCID: 0000-0002-4895-5936
Khaled A. Abdel-Sater – MD, Prof. of Physiology, Department of Dental and Medical Sciences, Faculty of Dentistry, Mutah University. E-mail: Kabdelsater@mutah.edu.jo; ORCID: 0000-0001-9357-4983; Scopus ID: 36112857600
Халед А. Абдель-Сатер – д-р медицины, проф. физиологии, каф. стоматологии и медицинских наук стоматологического фак-та Университета Мута. E-mail: kabdelsater@yahoo.com; ORCID: 0000-0001-9357-4983; Scopus ID: 36112857600
Received: 14.11.2025
Revised: 21.11.2025
Accepted: 27.11.2025
Поступила в редакцию: 14.11.2025
Поступила после рецензирования: 21.11.2025
Принята к публикации: 27.11.2025
Список исп. литературыСкрыть список1. Papalamprakopoulou Z, Dey P, Frascati R, Fountzilas C. Pancreatic steatosis as a risk factor for pancreatic ductal adenocarcinoma: pathogenesis and clinical implications. Clin Transl Gastroenterol 2025;16(6):e00832. DOI: 10.14309/ctg.0000000000000832
2. Altinel D, Basturk O, Sarmiento JM et al. Lipomatous pseudohypertrophy of the pancreas: a clinicopathologically distinct entity. Pancreas 2010;39(3):392-7. DOI: 10.1097/MPA.0b013e3181bd2923
3. Caldart F, de Pretis N, Luchini C et al. Pancreatic steatosis and metabolic pancreatic disease: a new entity? Intern Emerg Med 2023;18(8):2199-208. DOI: 10.1007/s11739-023-03364-y
4. Mathur A, Marine M, Lu D et al. Nonalcoholic fatty pancreas disease. HPB (Oxford) 2007;9(4):312-8. DOI: 10.1080/13651820701504157
5. Nassir F, Rector RS, Hammoud GM et al. Pathogenesis and prevention of hepatic steatosis. Gastroenterol Hepatol (N Y) 2015;11(3):167-75.
6. Rinella ME, Lazarus JV, Ratziu V et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol 2023;79(6):1542-56. DOI: 10.1016/j.jhep.2023.06.003
7. Stamm BH. Incidence and diagnostic significance of minor pathologic changes in the adult pancreas at autopsy: a systematic study of 112 autopsies in patients without known pancreatic disease. Hum Pathol 1984;15:677-83. DOI: 10.1016/s0046-8177(84)80294-4
8. Ye J, Wang JG, Liu RQ et al. Association between intra-pancreatic fat deposition and diseases of the exocrine pancreas: a narrative review. World J Gastroenterol 2025;31(2):101180. DOI: 10.3748/wjg.v31.i2.101180
9. Otsuka N, Shimamatsu Y, Hakuta R et al. Fatty pancreas: its potential as a risk factor for pancreatic cancer and clinical implications. Cancers (Basel) 2025;17(11):1765. DOI: 10.3390/cancers17111765
10. Chang ML. Fatty pancreas-centered metabolic basis of pancreatic adenocarcinoma: from obesity, diabetes and pancreatitis to oncogenesis. Biomedicines 2022;10(3):692. DOI: 10.3390/biomedicines10030692
11. Lee JS, Kim SH, Jun DW et al. Clinical implications of fatty pancreas: correlations between fatty pancreas and metabolic syndrome. World J Gastroenterol 2009;15(15):1869-75. DOI: 10.3748/wjg.15.1869
12. Wu WC, Wang CY. Association between non-alcoholic fatty pancreatic disease (NAFPD) and the metabolic syndrome: case-control retrospective study. Cardiovasc Diabetol 2013;12:77. DOI: 10.1186/1475-2840-12-77
13. Lim S, Meigs JB. Links between ectopic fat and vascular disease in humans. Arterioscler Thromb Vasc Biol 2014;34(9):1820-6. DOI: 10.1161/ATVBAHA.114.303035
14. Catanzaro R, Cuffari B, Italia A, Marotta F. Exploring the metabolic syndrome: nonalcoholic fatty pancreas disease. World J Gastroenterol 2016;22(34):7660-75. DOI: 10.3748/wjg.v22.i34.7660
15. Matsuda A, Makino N, Tozawa T et al. Pancreatic fat accumulation, fibrosis, and acinar cell injury in the Zucker diabetic fatty rat fed a chronic high-fat diet. Pancreas 2014;43(5):735-43. DOI: 10.1097/MPA.0000000000000129
16. Finelli C, Padula MC, Martelli G, Tarantino G. Could the improvement of obesity-related co-morbidities depend on modified gut hormones secretion? World J Gastroenterol 2014;20(44):16649-64. DOI: 10.3748/wjg.v20.i44.16649
17. Pagkali A, Makris A, Brofidi K et al. Pathophysiological mechanisms and clinical associations of non-alcoholic fatty pancreas disease. Diabetes Metab Syndr Obes 2024;17:283-94. DOI: 10.2147/DMSO.S397643
18. Idilman IS, Yildiz AE, Karaosmanoglu AD et al. Proton density fat fraction: magnetic resonance imaging applications beyond the liver. Diagn Interv Radiol 2022;28(1):83-91. DOI: 10.5152/dir.2021.21845
19. Hu HH, Kim HW, Nayak KS, Goran MI. Comparison of fat-water MRI and single-voxel MRS in the assessment of hepatic and pancreatic fat fractions in humans. Obesity (Silver Spring) 2010;18(4):841-7. DOI: 10.1038/oby.2009.352
20. Tanabe M, Higashi M, Tanabe M et al. Automated whole-volume measurement of CT fat fraction of the pancreas: correlation with Dixon MR imaging. Br J Radiol 2023;96(1146):20220937. DOI: 10.1259/bjr.20220937
21. Kim SY, Kim H, Cho JY et al. Quantitative assessment of pancreatic fat by using unenhanced CT: pathologic correlation and clinical implications. Radiology 2014;271(1):104-12. DOI: 10.1148/radiol.13122883
22. Jeong HT, Lee MS, Kim MJ. Quantitative analysis of pancreatic echogenicity on transabdominal sonography: correlations with metabolic syndrome. J Clin Ultrasound 2015;43(2):98-108. DOI: 10.1002/jcu.22200
23. Lesmana CRA, Ho KY, Lesmana LA. Impact of endoscopic ultrasound procedures in various pancreatobiliary disorders in Indonesia based on a case series in a private hospital. Case Rep Gastroenterol 2015;9:206-14. DOI: 10.1159/000431308
24. Larghia A, Petroneb MC, Galassoa D, Arcidiacono PG. Endoscopic ultrasound in the evaluation of pancreatobiliary disorders. Dig Liver Dis 2010;42:6-15. DOI: 10.1016/j.dld.2009.06.021
25. Sepe PS, Ohri A, Sanaka S et al. A prospective evaluation of fatty pancreas by using EUS. Gastrointest Endosc 2011;73:987-93. DOI: 10.1016/j.gie.2011.01.015
26. Shen F, Zheng RD, Mi YQ et al. Controlled attenuation parameter for non-invasive assessment of hepatic steatosis in Chinese patients. World J Gastroenterol 2014;20(16):4702-11. DOI: 10.3748/wjg.v20.i16.4702
27. Olsen TS. Lipomatosis of the pancreas in autopsy material and its relation to age and overweight. Acta Pathol Microbiol Scand A 1978;86A(5):367-73. DOI: 10.1111/j.1699-0463.1978.tb02058.x
28. Zheng Z, Zong Y, Ma Y et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther 2024;9:234. DOI: 10.1038/s41392-024-01931-z
29. Flint A, Andersen G, Hockings P et al. Randomised clinical trial: semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment Pharmacol Ther 2021;54(9):1150-61. DOI: 10.1111/apt.16608
30. Kuriyama T, Ishibashi C, Kozawa J et al. Effects of liraglutide on intrapancreatic fat deposition in patients with type 2 diabetes. Clin Nutr ESPEN 2024;59:208-13. DOI: 10.1016/j.clnesp.2023.12.005
31. Alharbi SH. Anti-inflammatory role of glucagon-like peptide 1 receptor agonists and its clinical implications. Ther Adv Endocrinol Metab 2024;15:20420188231222367. DOI: 10.1177/20420188231222367
32. Luo Y, Yang S, Zeng H et al. Both subcutaneous semaglutide and calorie restriction improve pancreatic cell hyperplasia and gut microbiota in high-fat diet-induced obese mice. Nutr Metab (Lond) 2025;22(1):95. DOI: 10.1186/s12986-025-00987-0
33. Neeland IJ, Marso SP, Ayers CR et al. Effects of liraglutide on visceral and ectopic fat in adults with overweight and obesity at high cardiovascular risk: a randomised, double-blind, placebo-controlled clinical trial. Lancet Diabetes Endocrinol 2021;9(9):595-605. DOI: 10.1016/S2213-8587(21)00179-0
34. Souza M, Al-Sharif L, Khalil SM, Diaz I. Placebo effect on changes in magnetic resonance-based endpoints in patients with MASH: systematic review and meta-analysis. J Clin Exp Hepatol 2025;15(6):103173. DOI: 10.1016/j.jceh.2025.103173
35. Maretty L, Gill D, Simonsen L et al. Proteomic changes upon treatment with semaglutide in individuals with obesity. Nat Med 2025;31:267-77. DOI: 10.1038/s41591-024-03355-2
36. Dankner R, Murad H, Agay N et al. Glucagon-like peptide-1 receptor agonists and pancreatic cancer risk in patients with type 2 diabetes. JAMA Netw Open 2024;7:e2350408. DOI: 10.1001/jamanetworkopen.2023.50408
37. Dore DD, Bloomgren GL, Wenten M et al. A cohort study of acute pancreatitis in relation to exenatide use. Diabetes Obes Metab. 2011;13:559-66.
38. Romley JA, Goldman DP, Solomon M et al. Exenatide therapy and the risk of pancreatitis and pancreatic cancer in a privately insured population. Diabetes Technol Ther 2012;14:904. DOI: 10.1089/dia.2012.0075
39. Wenten M, Gaebler JA, Hussein M et al. Relative risk of acute pancreatitis in initiators of exenatide twice daily compared with other anti-diabetic medication: a follow-up study. Diabet Med 2012;29:1412.
40. Elashoff M, Matveyenko AV, Gier B et al. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology 2011;141:150-6.
41. Lando HM, Alattar M, Dua AP. Elevated amylase and lipase levels in patients using glucagon-like peptide-1 receptor agonists or dipeptidyl-peptidase-4 inhibitors in the outpatient setting. Endocr Pract 2012;18:472-7.
42. Singh S, Chang HY, Richards TM et al. Glucagon-like peptide-1-based therapies and risk of hospitalization for acute pancreatitis in type 2 diabetes mellitus: a population-based matched case-control study. JAMA Intern Med 2013;173:534-9.
43. Meier JJ, Nauck MA. Risk of pancreatitis in patients treated with incretin-based therapies. Diabetologia 2014;57:1320-4.
44. Faour O, Boktor M, Yau H et al. GLP-1 receptor agonists initiation and risk of acute pancreatitis and pancreatic cancer: a real-world comparative study. Am J Med Open 2025;14:100114. DOI: 10.1016/j.ajmo.2025.100114
45. Ayoub M, Chela H, Amin N et al. Pancreatitis risk associated with GLP-1 receptor agonists, considered as a single class, in a comorbidity-free subgroup of type 2 diabetes patients in the United States: a propensity score-matched analysis. J Clin Med 2025;14(3):944. DOI: 10.3390/jcm14030944