Клинический разбор в общей медицине №05 2026
Университет Мута, Аль-Карак, Иордания
Kabdelsater@mutah.edu.jo
Аннотация
Синдром постуральной ортостатической тахикардии (СПОТ) – это широко распространенный инвалидизирующий компонент постковидного синдрома. Его разнообразные проявления, а именно – дисфункция вегетативной нервной системы, сердечно-сосудистой и иммунной систем, позволяют предположить наличие системной, а не изолированной патологии. Традиционно используемые модели отдельных путей не могут объяснить персистенцию и взаимосвязь этих симптомов.
Цель. В настоящей работе представлена модель гомеостатической нестабильности (Homeostatic Instability Model, HIM) как объединяющая основа для концептуализации постковидного СПОТ – системного биологического феномена, характеризуемого крахом общей физиологической устойчивости.
Материалы и методы. Выполнен всесторонний анализ литературы – прошедших рецензирование результатов исследований, опубликованных с января 2020 г. по октябрь 2025 г. Данные о вегетативной регуляции, активации иммунной системы, эндотелиальной функции и митохондриальном метаболизме были объединены с целью определить включающиеся раз за разом механизмы обратной связи, которые являются движущей силой хронического вегетативного расстройства.
Результаты. HIM описывает, как вызванная SARS-CoV-2 инфекция запускает самоусиливающиеся циклы дисфункции, в которые вовлечены опосредованная аутоантителами рецепторная сигнализация, эндотелиальная дисфункция, связанная с нарушением микроциркуляции гипоксия и митохондриальный окислительный стресс. Указанные процессы дестабилизируют вегетативную регуляцию и энергетический гомеостаз, препятствуя восстановлению физиологического равновесия. Клиническими проявлениями такой нестабильности являются ортостатическая гипотензия, тахикардия, общее недомогание и когнитивные нарушения.
Заключение. Модель гомеостатической нестабильности позволяет изменить концепцию постковидного СПОТ – с состояния с определенными симптомами на системное нарушение устойчивости. Она подчеркивает важность восстановления общей стабильности посредством применения комплексных мер, направленных на нормализацию работы вегетативной нервной системы, восстановление эндотелия и метаболического баланса, вместо подавления симптомов. HIM создает механистическую основу для разработки диагностических и терапевтических средств для восстановления согласованности функционирования систем организма при поствирусных вегетативных расстройствах.
Ключевые слова: лонг-ковид, СПОТ, адаптационная медицина, системная интеграция, общая физиология, поствирусное вегетативное расстройство.
Для цитирования: Абдель-Сатер Х.А. Модель гомеостатической нестабильности: переосмысление постковидного синдрома постуральной ортостатической тахикардии как ослабления устойчивости на системном уровне. Клинический разбор в общей медицине. 2026; 7 (4): 57–62. DOI: 10.47407/kr2026.7.5.00841
Introduction
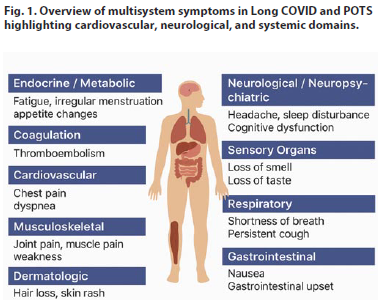
The coronavirus disease 2019 (COVID-19) pandemic has revealed a broad spectrum of post-acute sequelae, collectively termed Long COVID, characterized by persistent, multi-organ dysfunction beyond four weeks after infection. Among its most debilitating manifestations is Postural Orthostatic Tachycardia Syndrome (POTS) – a measurable form of autonomic dysregulation manifesting as orthostatic intolerance, tachycardia (≥30 bpm in adults), dyspnea, chest pain, fatigue, and cognitive impairment [1] (Fig. 1).
 Post-COVID-19 POTS affects approximately 2–14% of survivors and up to 61% of patients attending post-acute sequelae clinics [2], corresponding to an estimated global burden of 500,000 – 3 million cases [3]. The overall prevalence of Long COVID varies globally – 35% in Asia, 39% in Europe, 30% in North America, and 51% in South America – and remains substantial over time, persisting in 35% of individuals at one year and nearly 47% after two years [4]. Such variability reflects differences in study design, population characteristics, and healthcare access, as well as the influence of viral variants and vaccination status. Reported risk factors for both Long COVID and POTS include severe acute infection, older age, female sex, lack of vaccination, and infection by early SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) variants [5].
Post-COVID-19 POTS affects approximately 2–14% of survivors and up to 61% of patients attending post-acute sequelae clinics [2], corresponding to an estimated global burden of 500,000 – 3 million cases [3]. The overall prevalence of Long COVID varies globally – 35% in Asia, 39% in Europe, 30% in North America, and 51% in South America – and remains substantial over time, persisting in 35% of individuals at one year and nearly 47% after two years [4]. Such variability reflects differences in study design, population characteristics, and healthcare access, as well as the influence of viral variants and vaccination status. Reported risk factors for both Long COVID and POTS include severe acute infection, older age, female sex, lack of vaccination, and infection by early SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) variants [5].
Importantly, post-COVID-19 POTS is a distinct clinical entity rather than a simple recurrence of classic POTS. Evidence suggests that it arises from systemic dysregulation involving crosstalk between autonomic, immune, endothelial, and metabolic systems [6]. Mechanistic contributors include autoantibody-mediated G-protein-coupled receptor dysfunction [7], viral persistence and neuro-inflammation [2], angiotensin-converting enzyme 2 (ACE2)-related endothelial injury [8], renin-angiotensin-aldosterone system (RAAS) dysregulation [9], and gut–brain axis disruption [10]. These interconnected disruptions point toward a broader systems collapse – forming the basis of the proposed Homeostatic Instability Model (HIM).
Despite progress in identifying these mechanisms, current therapies targeting isolated pathways have shown limited benefit, underscoring the need for an integrative model that explains how these multi-system disturbances converge and perpetuate chronic physiological disequilibrium.
Accordingly, this article aims to: define the conceptual foundation of the HIM as a unifying systems framework describing how autonomic, immune, endothelial, and metabolic networks lose adaptive control following SARS-CoV-2 infection. Elucidate the feedback-loop architecture through which viral-induced perturbations sustain chronic autonomic dysfunction, trapping the body in a maladaptive equilibrium. And reorient diagnostic and therapeutic strategies toward restoring system resilience rather than suppressing isolated symptoms, promoting integrative interventions that recalibrate dysregulated physiological axes.
Materials and methods
A narrative review was conducted to synthesize the evolving literature on post-COVID-19 POTS. PubMed, Scopus, and Web of Science were systematically searched for English-language articles published between January 2020 and October 2025 using combinations of the terms “Postural Orthostatic Tachycardia Syndrome,” “POTS,” “dysautonomia,” “SARS-CoV-2,” and “COVID-19.” Inclusion criteria comprised original peer-reviewed studies involving adults or adolescents with post-COVID dysautonomia, while non–peer-reviewed articles, editorials, and purely theoretical commentaries were excluded.
A narrative synthesis was chosen over a systematic review due to the mechanistic heterogeneity and early stage of evidence, with the primary goal of integrating findings from basic science, translational models, and clinical observations into a coherent conceptual framework rather than performing a quantitative meta-analysis; accordingly, formal systematic review standards (e.g., PRISMA) and risk-of-bias assessments were not applied.
While this approach may limit replicability, it enhances conceptual synthesis by enabling cross-disciplinary integration. To minimize bias, only high-quality, peer-reviewed studies were prioritized, emphasizing mechanistic consistency across independent reports. Given the rapidly evolving evidence base, the proposed HIM should be regarded as a dynamic framework, open to ongoing validation and refinement in future research.
 Results and discussion
Results and discussion
Mechanistic foundations of the homeostatic instability model
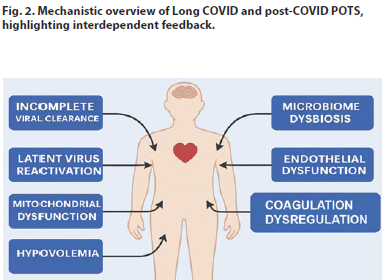
Long COVID arises from interdependent mechanisms – viral persistence, immune dysregulation, endothelial dysfunction, and metabolic failure – that form self-reinforcing feedback loops sustaining maladaptive physiology (Fig. 2). These processes interact to create cycles of inflammation, tissue injury, and autonomic instability that underpin chronic symptoms [11]. These interlocked loops – illustrated in Fig. 2 – form the core of the HIM framework.
1. Infectious persistence loop
Incomplete viral clearance is supported by the detection of SARS-CoV-2 RNA and proteins in blood, feces, and tissues up to 12 months’ post-infection [12]. Persistent antigens, especially the SARS-CoV-2 spike protein, can drive ongoing immune activation by triggering NOD-, LRR- and pyrin domain-containing protein 3 (NLRP3)-mediated pro-inflammatory signaling and promoting interleukin-1 beta (IL-1β) production [13]. Impaired viral clearance likely reflects immune evasion, cluster of differentiation 8 positive (CD8+) T cell exhaustion, and viral persistence within immunologically tolerant niches such as the gut [14]. Latent virus reactivation – particularly Epstein–Barr virus and human herpesvirus 6 (HHV-6) – occurs in up to 40% of Long COVID patients, contributing to fatigue and neuropsychiatric symptoms [15]. SARS-CoV-2-mediated interferon suppression promotes reactivation, while EBV may reciprocally enhance SARS-CoV-2 infectivity by upregulating ACE2, inducing chronic inflammation and potentially triggering autoimmunity [16].
2. Immune–autonomic cross-talk
Immune dysregulation and autoimmunity are central mechanisms. Long COVID patients demonstrate persistent T-cell activation, reduced natural killer cell cytotoxicity, and prolonged antigen-driven inflammation [17]. Molecular mimicry, bystander activation, and epitope spreading may explain the emergence of autoantibodies targeting adrenergic, cholinergic, and endothelial receptors, driving neurological and cardiovascular dysfunction [18].
3. Gut–brain axis disruption
SARS-CoV-2-induced gut dysbiosis amplifies systemic inflammation. Intestinal epithelial disruption reduces beneficial bacteria (e.g., Faecalibacterium, Bifidobacterium) and enriches proinflammatory taxa (e.g., Enterococcus) [19]. Loss of short-chain fatty acids such as butyrate impairs barrier integrity, promotes T helper 17 / Regulatory T cell imbalance, and contributes to neuroinflammation and fatigue [20].
4. Endothelial–mitochondrial coupling failure
Endothelial injury. Persistent endothelial dysfunction and coagulation abnormalities produce sustained microvascular injury and thrombosis. Complement activation degrades the endothelial glycocalyx, increases von Willebrand factor and Factor VIII, creating a prothrombotic milieu [21]. Platelet–neutrophil aggregates and neutrophil extracellular trap formation maintain vascular inflammation and microthrombosis, correlating with cognitive and cardiovascular symptoms [22].
Mitochondrial dysfunction. Impaired oxidative phosphorylation shifts energy metabolism toward anaerobic pathways, explaining post-exertional malaise and cognitive fatigue [23]. Mitochondrial oxidative stress activates nuclear factor kappa-B (NF-κB) , linking metabolic failure with chronic inflammation [24]. SARS-CoV-2 proteins disrupt mitochondrial antiviral signaling, further impairing energy metabolism and immune balance [25].
Cross-talk failure. Endothelial and mitochondrial dysfunction interact to exacerbate systemic instability, contributing to persistent autonomic and metabolic dysregulation.
5. RAAS and fluid dynamics breakdown
Integrating these findings, the HIM conceptualizes post-COVID POTS as a cascade of interdependent feedback loops leading to systemic instability. Autoantibodies targeting adrenergic and cholinergic receptors, RAAS imbalance, endothelial injury, and brainstem involvement collectively impair autonomic regulation, producing hallmark POTS symptoms [15]. Secondary stressors – cytokine storms, dehydration, and deconditioning – exacerbate hypovolemia and sympathetic overdrive [10].
Post-COVID POTS may result from low blood volume and a deconditioned heart. Fever and prolonged bed rest contribute to hypovolemia and cardiovascular deconditioning, while RAAS dysfunction – characterized by low renin and aldosterone despite low blood volume – reflects ACE2 disruption and impaired fluid homeostasis. Compensatory tachycardia arises in response to reduced stroke volume [26].
The HIM framework emphasizes that Long COVID is not a single-organ disorder but a systems biology condition driven by interlocking mechanisms of immune, metabolic, endothelial, and autonomic dysregulation [27]. By conceptualizing these interdependent feedback loops, HIM provides a mechanistic foundation for understanding chronic dysautonomia and guiding resilience-focused interventions.
Towards a new diagnostics: biomarkers and multi-system assessment of systemic resilience
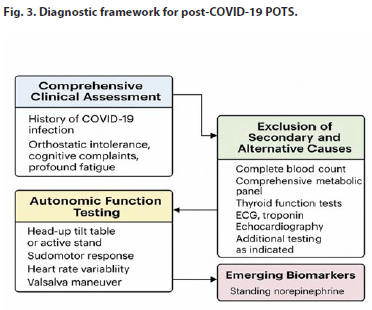
Diagnosing post-COVID-19 POTS is challenging due to symptom overlap with other post-viral fatigue and autonomic syndromes, necessitating a structured, multi-dimensional framework. A stepwise approach – integrating clinical assessment, exclusion of secondary causes, confirmatory autonomic testing, and biomarker exploration – is essential [10] (Fig. 3).
 1. Comprehensive clinical assessment
1. Comprehensive clinical assessment
Diagnosis begins with a detailed clinical evaluation, focusing on the temporal link between SARS-CoV-2 infection and symptom onset. Key manifestations – including orthostatic intolerance, palpitations, fatigue, cognitive dysfunction (“brain fog”), and lightheadedness – should be documented as a unified symptom cluster, noting triggers and diurnal variability [1]. Medications affecting heart rate or autonomic tone (e.g., beta-blockers, anticholinergics, or adrenergic stimulants) must be reviewed to prevent confounding results. This groundwork supports subsequent objective testing and helps differentiate POTS from other autonomic or cardiovascular disorders [28].
2. Exclusion of secondary and alternative etiologies
Systematic exclusion of secondary causes and mimicking disorders is pivotal. Laboratory evaluations typically include complete blood count, comprehensive metabolic panel, and thyroid function to rule out anemia, electrolyte disturbances, and thyroid dysfunction [2].
Additional assessments – morning cortisol, plasma catecholamines, and 24-hour urinary sodium – detect adrenal or volume-regulatory abnormalities [29]. Cardiopulmonary symptoms warrant electrocardiogram (ECG), serum troponin, and transthoracic echocardiography to exclude structural heart disease or myocarditis, with advanced imaging [cardiac magnetic resonance imaging (MRI) or computed tomography (CT) pulmonary angiography] as needed [12]. This ensures that a POTS diagnosis reflects a primary dysautonomic mechanism rather than secondary systemic illness.
3. Autonomic function testing and diagnostic confirmation
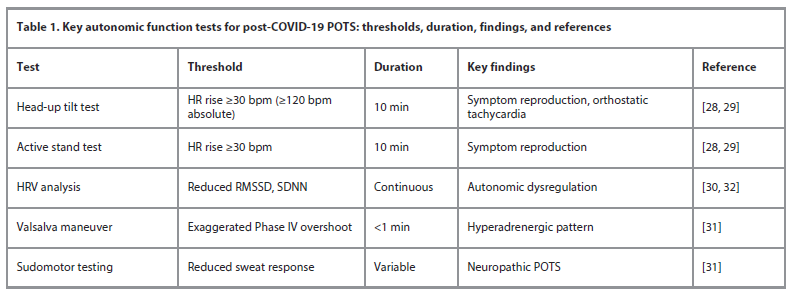
After excluding secondary causes, autonomic testing is central to confirming post-COVID-19 POTS. The head-up tilt test or active standing test detects orthostatic heart rate abnormalities and reproduces characteristic symptoms [28]. Diagnostic criteria include a sustained HR increase ≥30 bpm (or ≥120 bpm absolute) within 10 minutes of standing without orthostatic hypotension, alongside symptom reproduction [29]. Complementary assessments – heart rate variability, Valsalva maneuver, and sudomotor testing – further delineate autonomic integrity [30].
Table 1 summarizes key autonomic tests, thresholds, duration, characteristic findings, and references for clinical practice. Measurement of standing plasma catecholamines supports phenotyping into hyperadrenergic, neuropathic, or hypovolemic subtypes, which carry distinct therapeutic implications [16, 31]. Multimodal testing – including continuous tilt monitoring, 24-hour ECG, ambulatory blood pressure monitoring, exercise ECG, echocardiography, and specialized autonomic tests – enhances diagnostic precision [32, 33].
4. Emerging biomarkers and mechanistic mapping
Biomarker discovery is expanding mechanistic insights into post-COVID-19 POTS [31]. Candidate biomarkers include elevated standing norepinephrine (hyperadrenergic phenotype), persistent proinflammatory cytokines (immune activation), and functional autoantibodies against adrenergic and muscarinic receptors (autoimmune dysautonomia) [15].
These biomarkers align with the HIM: autoantibodies reflect immune feedback loop disruption, cytokine patterns indicate inflammatory loops, and norepinephrine dysregulation represents autonomic loops. Integrating molecular data with clinical and physiological assessments moves diagnosis from exclusion toward mechanistic specificity, enabling precision-targeted interventions.
5. Toward an integrated diagnostic pathway
The optimal diagnostic approach layers: (1) comprehensive clinical assessment, (2) exclusion of secondary causes, (3) autonomic testing, and (4) incorporation of biomarker or imaging data where available. This structured framework maximizes diagnostic accuracy and supports early identification of post-COVID-19 autonomic sequelae [34]. A unified model bridging bedside evaluation with emerging molecular diagnostics provides a foundation for personalized management of post-COVID-19 POTS [35].
Therapeutic approaches: multimodal resilience restoration
Management of post-COVID-19 POTS requires a multidisciplinary, phenotype-based approach, integrating lifestyle, pharmacologic, and mechanistic-targeted strategies to restore autonomic and systemic resilience [36]. Treatment follows established POTS principles, emphasizing individualized care guided by clinical phenotype, biomarker profiles, and systemic assessment.
1. Lifestyle and non-pharmacologic interventions
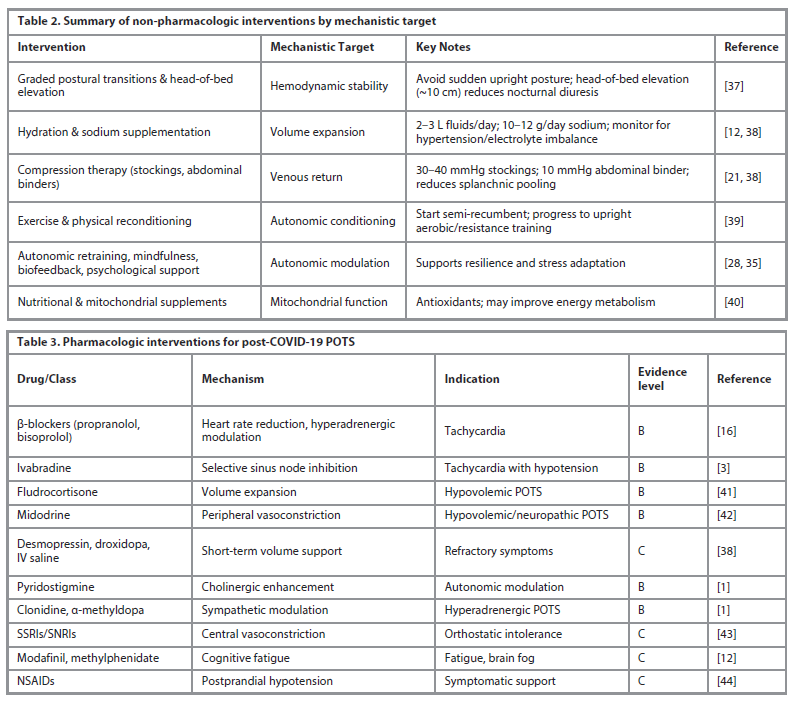
Key non-pharmacologic strategies target volume expansion, autonomic modulation, and mitochondrial support. Table 2 summarizes the main interventions and their mechanistic targets.
2. Pharmacologic management
Pharmacologic therapy is considered for patients with persistent debilitating symptoms, individualized according to phenotype (tachycardic, hypovolemic, hyperadrenergic). Table 3 classifies agents by mechanism and evidence strength.
3. Pathophysiology-targeted therapies
Therapies aimed at underlying mechanisms of Long COVID and POTS include:
Antiviral approaches. Persistent viral reservoirs may contribute to pathogenesis. Nirmatrelvir/ritonavir is under investigation for prolonged or personalized dosing [45].
Immunomodulatory therapies. Targeting IL-6, IL-1β, interferon, tumor necrosis factor, Janus Kinase (JAK) pathways (e.g., baricitinib, IVIG, plasmapheresis). Ongoing trials include baricitinib for neurocognitive impairment (REVERSE-LC; NCT06631287) [46].
Microbiota-targeted interventions: Gut dysbiosis influences systemic inflammation. Probiotics (e.g., Lactiplantibacillus plantarum 299v), multi-strain formulations (SIM01), and fecal microbiota transplantation are under investigation; prospective urban rural epidemiology – low-carbohydrate study (NCT06643299) examines long-term benefits [47].
Mitochondrial supportive therapies. Supplements such as antioxidants, creatine, pyrroloquinoline quinone, omega-3 fatty acids, and branched-chain amino acids support energy metabolism. Gut–mitochondria axis modulation through probiotics/prebiotics may further enhance outcomes [40].
Anticoagulation/antiplatelet therapy. Targeting microthrombosis and endothelial dysfunction. Short-term aspirin, clopidogrel, or apixaban may reduce microclot burden; therapy should be individualized based on coagulation/inflammation biomarkers [48].
4. Integrative and future directions
Management of POTS is increasingly framed as multimodal resilience restoration, addressing not only heart-rate control but systemic recalibration across autonomic, immune, endothelial, and metabolic domains [15]. Future strategies under investigation include vagal nerve stimulation, low-dose naltrexone, targeted antioxidants, and endothelial-protective agents.
Optimal outcomes emerge from multimodal synergy – combining low-dose pharmacotherapy, exercise reconditioning, cognitive-behavioral therapy, and metabolic optimization. This resilience-oriented framework holds promise for restoring adaptive homeostasis and improving long-term recovery in post-COVID-19 POTS.
A Roadmap for validation and future directions
Translating the HIM from conceptual framework to clinical utility requires a structured, multi-phase validation approach. Future research should begin with deep phenotyping and longitudinal studies tracking patients from acute infection through chronic phases, mapping the progression of systemic instability and identifying resilience biomarkers via multi-omics profiling and autonomic assessments.
Mechanistic investigations employing high-resolution physiological monitoring and computational modeling can clarify feedback loops among autonomic, immune, endothelial, and metabolic systems. Building on these insights, adaptive interventional trials should stratify patients according to their dominant instability profile – whether autoimmune, endothelial, or metabolic – and test targeted, multimodal therapies designed to restore systemic resilience. Success metrics should extend beyond symptom reduction to include objective restoration of physiological coherence across systems.
Collaborative, cross-disciplinary efforts integrating neurology, immunology, vascular biology, and systems physiology are essential to validate HIM and translate mechanistic understanding into clinical practice.
Ultimately, this work represents a systems-medicine shift – from symptom control to resilience engineering – which may redefine therapeutic goals for post-viral dysautonomia, aligning directly with the overarching theme of homeostatic instability and resilience failure.
Conclusion
Post-COVID-19 POTS illustrates how a transient viral insult can trigger chronic, systems-level failure. The HIM reframes POTS as a network pathology – an emergent collapse of interconnected autonomic, immune, endothelial, and metabolic loops – rather than a discrete autonomic defect. HIM explains why diverse findings – autoantibodies, hypovolemia, mitochondrial stress, microcirculatory dysfunction – converge into a single clinical phenotype and accounts for the relapsing, fluctuating nature of symptoms.
Therapeutically, this perspective shifts the focus from symptom suppression to resilience restoration, integrating pharmacologic modulation of adrenergic tone, endothelial protection, mitochondrial support, and neuroimmune recalibration with rehabilitation strategies encompassing autonomic retraining and metabolic conditioning.
For validation, HIM advocates a structured roadmap:
1. Quantify multi-axis instability via HRV, endothelial, immune, and metabolic biomarkers.
2. Apply network modeling to simulate recovery trajectories.
3. Conduct clinical trials assessing improvements in resilience indices rather than isolated parameters.
Operationalizing HIM through longitudinal biomarker panels and computational network mapping promises to establish a new diagnostic and therapeutic paradigm for post-viral dysautonomia.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the author
Информация об авторе
Khaled A. Abdel-Sater – MD, Prof. of Physiology, Faculty of Dentistry, Mutah University.
E-mail: Kabdelsater@mutah.edu.jo; ORCID: 0000-0001-9357-4983
Халед А. Абдель-Сатер – д-р медицины, проф. физиологии стоматологического фак-та Университета Мута. E-mail: Kabdelsater@mutah.edu.jo; ORCID: 0000-0001-9357-4983
Received: 10.10.2025
Revised: 30.10.2025
Accepted: 13.11.2025
Поступила в редакцию: 10.10.2025
Поступила после рецензирования: 30.10.2025
Принята к публикации: 13.11.2025
Клинический разбор в общей медицине №05 2026
The homeostatic instability model: reframing post-COVID-19 POTS as a systems-level failure of resilience
Номера страниц в выпуске:57-62
Abstract
Postural Orthostatic Tachycardia Syndrome (POTS) has emerged as a frequent and disabling component of post-coronavirus disease 2019 (post-COVID-19) syndrome. Its heterogeneous manifestations – spanning autonomic, cardiovascular, immunologic, and metabolic dysfunction – suggest a systems-level disturbance rather than an isolated disorder. Traditional single-pathway models cannot explain the persistence and interconnectivity of these symptoms.
Aim. This study introduces the Homeostatic Instability Model (HIM) as a unifying framework to conceptualize post-COVID-19 POTS as a systems biology phenomenon characterized by the collapse of integrated physiological resilience.
Materials and methods. A comprehensive literature synthesis was conducted using peer-reviewed studies published between January 2020 and October 2025. Evidence from autonomic regulation, immune activation, endothelial function, and mitochondrial metabolism was integrated to identify recurrent feedback loops driving chronic dysautonomia.
Results. The HIM describes how severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection initiates self-reinforcing cycles of dysfunction involving autoantibody-mediated receptor signaling, endothelial inflammation, microvascular hypoxia, and mitochondrial oxidative stress. These processes destabilize autonomic control and energy homeostasis, preventing recovery of physiological equilibrium. Clinically, this instability manifests as orthostatic intolerance, tachycardia, fatigue, and cognitive impairment.
Conclusion. The HIM reframes post-COVID-19 POTS from a symptom-based condition to a systemic resilience disorder. It emphasizes restoration of network stability through integrated interventions – targeting autonomic retraining, endothelial repair, and metabolic rebalancing – rather than symptomatic suppression. HIM provides a mechanistic basis for developing diagnostics and therapies aimed at rebuilding systemic coherence in post-viral dysautonomia.
Keywords: Long COVID, POTS, resilience medicine, systems integration, network physiology, post-viral dysautonomia.
For citation: Abdel-Sater Kh.A. The homeostatic instability model: reframing post-COVID-19 POTS as a systems-level failure of resilience. Clinical review for general practice. 2026; 7 (5): 57–62 (In Russ.). DOI: 10.47407/kr2026.7.5.00841
Postural Orthostatic Tachycardia Syndrome (POTS) has emerged as a frequent and disabling component of post-coronavirus disease 2019 (post-COVID-19) syndrome. Its heterogeneous manifestations – spanning autonomic, cardiovascular, immunologic, and metabolic dysfunction – suggest a systems-level disturbance rather than an isolated disorder. Traditional single-pathway models cannot explain the persistence and interconnectivity of these symptoms.
Aim. This study introduces the Homeostatic Instability Model (HIM) as a unifying framework to conceptualize post-COVID-19 POTS as a systems biology phenomenon characterized by the collapse of integrated physiological resilience.
Materials and methods. A comprehensive literature synthesis was conducted using peer-reviewed studies published between January 2020 and October 2025. Evidence from autonomic regulation, immune activation, endothelial function, and mitochondrial metabolism was integrated to identify recurrent feedback loops driving chronic dysautonomia.
Results. The HIM describes how severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection initiates self-reinforcing cycles of dysfunction involving autoantibody-mediated receptor signaling, endothelial inflammation, microvascular hypoxia, and mitochondrial oxidative stress. These processes destabilize autonomic control and energy homeostasis, preventing recovery of physiological equilibrium. Clinically, this instability manifests as orthostatic intolerance, tachycardia, fatigue, and cognitive impairment.
Conclusion. The HIM reframes post-COVID-19 POTS from a symptom-based condition to a systemic resilience disorder. It emphasizes restoration of network stability through integrated interventions – targeting autonomic retraining, endothelial repair, and metabolic rebalancing – rather than symptomatic suppression. HIM provides a mechanistic basis for developing diagnostics and therapies aimed at rebuilding systemic coherence in post-viral dysautonomia.
Keywords: Long COVID, POTS, resilience medicine, systems integration, network physiology, post-viral dysautonomia.
For citation: Abdel-Sater Kh.A. The homeostatic instability model: reframing post-COVID-19 POTS as a systems-level failure of resilience. Clinical review for general practice. 2026; 7 (5): 57–62 (In Russ.). DOI: 10.47407/kr2026.7.5.00841
Модель гомеостатической нестабильности: переосмысление постковидного синдрома постуральной ортостатической тахикардии как ослабления устойчивости на системном уровне
Халед А. Абдель-СатерУниверситет Мута, Аль-Карак, Иордания
Kabdelsater@mutah.edu.jo
Аннотация
Синдром постуральной ортостатической тахикардии (СПОТ) – это широко распространенный инвалидизирующий компонент постковидного синдрома. Его разнообразные проявления, а именно – дисфункция вегетативной нервной системы, сердечно-сосудистой и иммунной систем, позволяют предположить наличие системной, а не изолированной патологии. Традиционно используемые модели отдельных путей не могут объяснить персистенцию и взаимосвязь этих симптомов.
Цель. В настоящей работе представлена модель гомеостатической нестабильности (Homeostatic Instability Model, HIM) как объединяющая основа для концептуализации постковидного СПОТ – системного биологического феномена, характеризуемого крахом общей физиологической устойчивости.
Материалы и методы. Выполнен всесторонний анализ литературы – прошедших рецензирование результатов исследований, опубликованных с января 2020 г. по октябрь 2025 г. Данные о вегетативной регуляции, активации иммунной системы, эндотелиальной функции и митохондриальном метаболизме были объединены с целью определить включающиеся раз за разом механизмы обратной связи, которые являются движущей силой хронического вегетативного расстройства.
Результаты. HIM описывает, как вызванная SARS-CoV-2 инфекция запускает самоусиливающиеся циклы дисфункции, в которые вовлечены опосредованная аутоантителами рецепторная сигнализация, эндотелиальная дисфункция, связанная с нарушением микроциркуляции гипоксия и митохондриальный окислительный стресс. Указанные процессы дестабилизируют вегетативную регуляцию и энергетический гомеостаз, препятствуя восстановлению физиологического равновесия. Клиническими проявлениями такой нестабильности являются ортостатическая гипотензия, тахикардия, общее недомогание и когнитивные нарушения.
Заключение. Модель гомеостатической нестабильности позволяет изменить концепцию постковидного СПОТ – с состояния с определенными симптомами на системное нарушение устойчивости. Она подчеркивает важность восстановления общей стабильности посредством применения комплексных мер, направленных на нормализацию работы вегетативной нервной системы, восстановление эндотелия и метаболического баланса, вместо подавления симптомов. HIM создает механистическую основу для разработки диагностических и терапевтических средств для восстановления согласованности функционирования систем организма при поствирусных вегетативных расстройствах.
Ключевые слова: лонг-ковид, СПОТ, адаптационная медицина, системная интеграция, общая физиология, поствирусное вегетативное расстройство.
Для цитирования: Абдель-Сатер Х.А. Модель гомеостатической нестабильности: переосмысление постковидного синдрома постуральной ортостатической тахикардии как ослабления устойчивости на системном уровне. Клинический разбор в общей медицине. 2026; 7 (4): 57–62. DOI: 10.47407/kr2026.7.5.00841
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has revealed a broad spectrum of post-acute sequelae, collectively termed Long COVID, characterized by persistent, multi-organ dysfunction beyond four weeks after infection. Among its most debilitating manifestations is Postural Orthostatic Tachycardia Syndrome (POTS) – a measurable form of autonomic dysregulation manifesting as orthostatic intolerance, tachycardia (≥30 bpm in adults), dyspnea, chest pain, fatigue, and cognitive impairment [1] (Fig. 1).
Post-COVID-19 POTS affects approximately 2–14% of survivors and up to 61% of patients attending post-acute sequelae clinics [2], corresponding to an estimated global burden of 500,000 – 3 million cases [3]. The overall prevalence of Long COVID varies globally – 35% in Asia, 39% in Europe, 30% in North America, and 51% in South America – and remains substantial over time, persisting in 35% of individuals at one year and nearly 47% after two years [4]. Such variability reflects differences in study design, population characteristics, and healthcare access, as well as the influence of viral variants and vaccination status. Reported risk factors for both Long COVID and POTS include severe acute infection, older age, female sex, lack of vaccination, and infection by early SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) variants [5].Importantly, post-COVID-19 POTS is a distinct clinical entity rather than a simple recurrence of classic POTS. Evidence suggests that it arises from systemic dysregulation involving crosstalk between autonomic, immune, endothelial, and metabolic systems [6]. Mechanistic contributors include autoantibody-mediated G-protein-coupled receptor dysfunction [7], viral persistence and neuro-inflammation [2], angiotensin-converting enzyme 2 (ACE2)-related endothelial injury [8], renin-angiotensin-aldosterone system (RAAS) dysregulation [9], and gut–brain axis disruption [10]. These interconnected disruptions point toward a broader systems collapse – forming the basis of the proposed Homeostatic Instability Model (HIM).
Despite progress in identifying these mechanisms, current therapies targeting isolated pathways have shown limited benefit, underscoring the need for an integrative model that explains how these multi-system disturbances converge and perpetuate chronic physiological disequilibrium.
Accordingly, this article aims to: define the conceptual foundation of the HIM as a unifying systems framework describing how autonomic, immune, endothelial, and metabolic networks lose adaptive control following SARS-CoV-2 infection. Elucidate the feedback-loop architecture through which viral-induced perturbations sustain chronic autonomic dysfunction, trapping the body in a maladaptive equilibrium. And reorient diagnostic and therapeutic strategies toward restoring system resilience rather than suppressing isolated symptoms, promoting integrative interventions that recalibrate dysregulated physiological axes.
Materials and methods
A narrative review was conducted to synthesize the evolving literature on post-COVID-19 POTS. PubMed, Scopus, and Web of Science were systematically searched for English-language articles published between January 2020 and October 2025 using combinations of the terms “Postural Orthostatic Tachycardia Syndrome,” “POTS,” “dysautonomia,” “SARS-CoV-2,” and “COVID-19.” Inclusion criteria comprised original peer-reviewed studies involving adults or adolescents with post-COVID dysautonomia, while non–peer-reviewed articles, editorials, and purely theoretical commentaries were excluded.
A narrative synthesis was chosen over a systematic review due to the mechanistic heterogeneity and early stage of evidence, with the primary goal of integrating findings from basic science, translational models, and clinical observations into a coherent conceptual framework rather than performing a quantitative meta-analysis; accordingly, formal systematic review standards (e.g., PRISMA) and risk-of-bias assessments were not applied.
While this approach may limit replicability, it enhances conceptual synthesis by enabling cross-disciplinary integration. To minimize bias, only high-quality, peer-reviewed studies were prioritized, emphasizing mechanistic consistency across independent reports. Given the rapidly evolving evidence base, the proposed HIM should be regarded as a dynamic framework, open to ongoing validation and refinement in future research.
Results and discussionMechanistic foundations of the homeostatic instability model
Long COVID arises from interdependent mechanisms – viral persistence, immune dysregulation, endothelial dysfunction, and metabolic failure – that form self-reinforcing feedback loops sustaining maladaptive physiology (Fig. 2). These processes interact to create cycles of inflammation, tissue injury, and autonomic instability that underpin chronic symptoms [11]. These interlocked loops – illustrated in Fig. 2 – form the core of the HIM framework.
1. Infectious persistence loop
Incomplete viral clearance is supported by the detection of SARS-CoV-2 RNA and proteins in blood, feces, and tissues up to 12 months’ post-infection [12]. Persistent antigens, especially the SARS-CoV-2 spike protein, can drive ongoing immune activation by triggering NOD-, LRR- and pyrin domain-containing protein 3 (NLRP3)-mediated pro-inflammatory signaling and promoting interleukin-1 beta (IL-1β) production [13]. Impaired viral clearance likely reflects immune evasion, cluster of differentiation 8 positive (CD8+) T cell exhaustion, and viral persistence within immunologically tolerant niches such as the gut [14]. Latent virus reactivation – particularly Epstein–Barr virus and human herpesvirus 6 (HHV-6) – occurs in up to 40% of Long COVID patients, contributing to fatigue and neuropsychiatric symptoms [15]. SARS-CoV-2-mediated interferon suppression promotes reactivation, while EBV may reciprocally enhance SARS-CoV-2 infectivity by upregulating ACE2, inducing chronic inflammation and potentially triggering autoimmunity [16].
2. Immune–autonomic cross-talk
Immune dysregulation and autoimmunity are central mechanisms. Long COVID patients demonstrate persistent T-cell activation, reduced natural killer cell cytotoxicity, and prolonged antigen-driven inflammation [17]. Molecular mimicry, bystander activation, and epitope spreading may explain the emergence of autoantibodies targeting adrenergic, cholinergic, and endothelial receptors, driving neurological and cardiovascular dysfunction [18].
3. Gut–brain axis disruption
SARS-CoV-2-induced gut dysbiosis amplifies systemic inflammation. Intestinal epithelial disruption reduces beneficial bacteria (e.g., Faecalibacterium, Bifidobacterium) and enriches proinflammatory taxa (e.g., Enterococcus) [19]. Loss of short-chain fatty acids such as butyrate impairs barrier integrity, promotes T helper 17 / Regulatory T cell imbalance, and contributes to neuroinflammation and fatigue [20].
4. Endothelial–mitochondrial coupling failure
Endothelial injury. Persistent endothelial dysfunction and coagulation abnormalities produce sustained microvascular injury and thrombosis. Complement activation degrades the endothelial glycocalyx, increases von Willebrand factor and Factor VIII, creating a prothrombotic milieu [21]. Platelet–neutrophil aggregates and neutrophil extracellular trap formation maintain vascular inflammation and microthrombosis, correlating with cognitive and cardiovascular symptoms [22].
Mitochondrial dysfunction. Impaired oxidative phosphorylation shifts energy metabolism toward anaerobic pathways, explaining post-exertional malaise and cognitive fatigue [23]. Mitochondrial oxidative stress activates nuclear factor kappa-B (NF-κB) , linking metabolic failure with chronic inflammation [24]. SARS-CoV-2 proteins disrupt mitochondrial antiviral signaling, further impairing energy metabolism and immune balance [25].
Cross-talk failure. Endothelial and mitochondrial dysfunction interact to exacerbate systemic instability, contributing to persistent autonomic and metabolic dysregulation.
5. RAAS and fluid dynamics breakdown
Integrating these findings, the HIM conceptualizes post-COVID POTS as a cascade of interdependent feedback loops leading to systemic instability. Autoantibodies targeting adrenergic and cholinergic receptors, RAAS imbalance, endothelial injury, and brainstem involvement collectively impair autonomic regulation, producing hallmark POTS symptoms [15]. Secondary stressors – cytokine storms, dehydration, and deconditioning – exacerbate hypovolemia and sympathetic overdrive [10].
Post-COVID POTS may result from low blood volume and a deconditioned heart. Fever and prolonged bed rest contribute to hypovolemia and cardiovascular deconditioning, while RAAS dysfunction – characterized by low renin and aldosterone despite low blood volume – reflects ACE2 disruption and impaired fluid homeostasis. Compensatory tachycardia arises in response to reduced stroke volume [26].
The HIM framework emphasizes that Long COVID is not a single-organ disorder but a systems biology condition driven by interlocking mechanisms of immune, metabolic, endothelial, and autonomic dysregulation [27]. By conceptualizing these interdependent feedback loops, HIM provides a mechanistic foundation for understanding chronic dysautonomia and guiding resilience-focused interventions.
Towards a new diagnostics: biomarkers and multi-system assessment of systemic resilience
Diagnosing post-COVID-19 POTS is challenging due to symptom overlap with other post-viral fatigue and autonomic syndromes, necessitating a structured, multi-dimensional framework. A stepwise approach – integrating clinical assessment, exclusion of secondary causes, confirmatory autonomic testing, and biomarker exploration – is essential [10] (Fig. 3).
1. Comprehensive clinical assessmentDiagnosis begins with a detailed clinical evaluation, focusing on the temporal link between SARS-CoV-2 infection and symptom onset. Key manifestations – including orthostatic intolerance, palpitations, fatigue, cognitive dysfunction (“brain fog”), and lightheadedness – should be documented as a unified symptom cluster, noting triggers and diurnal variability [1]. Medications affecting heart rate or autonomic tone (e.g., beta-blockers, anticholinergics, or adrenergic stimulants) must be reviewed to prevent confounding results. This groundwork supports subsequent objective testing and helps differentiate POTS from other autonomic or cardiovascular disorders [28].
2. Exclusion of secondary and alternative etiologies
Systematic exclusion of secondary causes and mimicking disorders is pivotal. Laboratory evaluations typically include complete blood count, comprehensive metabolic panel, and thyroid function to rule out anemia, electrolyte disturbances, and thyroid dysfunction [2].
Additional assessments – morning cortisol, plasma catecholamines, and 24-hour urinary sodium – detect adrenal or volume-regulatory abnormalities [29]. Cardiopulmonary symptoms warrant electrocardiogram (ECG), serum troponin, and transthoracic echocardiography to exclude structural heart disease or myocarditis, with advanced imaging [cardiac magnetic resonance imaging (MRI) or computed tomography (CT) pulmonary angiography] as needed [12]. This ensures that a POTS diagnosis reflects a primary dysautonomic mechanism rather than secondary systemic illness.
3. Autonomic function testing and diagnostic confirmation
After excluding secondary causes, autonomic testing is central to confirming post-COVID-19 POTS. The head-up tilt test or active standing test detects orthostatic heart rate abnormalities and reproduces characteristic symptoms [28]. Diagnostic criteria include a sustained HR increase ≥30 bpm (or ≥120 bpm absolute) within 10 minutes of standing without orthostatic hypotension, alongside symptom reproduction [29]. Complementary assessments – heart rate variability, Valsalva maneuver, and sudomotor testing – further delineate autonomic integrity [30].
Table 1 summarizes key autonomic tests, thresholds, duration, characteristic findings, and references for clinical practice. Measurement of standing plasma catecholamines supports phenotyping into hyperadrenergic, neuropathic, or hypovolemic subtypes, which carry distinct therapeutic implications [16, 31]. Multimodal testing – including continuous tilt monitoring, 24-hour ECG, ambulatory blood pressure monitoring, exercise ECG, echocardiography, and specialized autonomic tests – enhances diagnostic precision [32, 33].
4. Emerging biomarkers and mechanistic mapping
Biomarker discovery is expanding mechanistic insights into post-COVID-19 POTS [31]. Candidate biomarkers include elevated standing norepinephrine (hyperadrenergic phenotype), persistent proinflammatory cytokines (immune activation), and functional autoantibodies against adrenergic and muscarinic receptors (autoimmune dysautonomia) [15].
These biomarkers align with the HIM: autoantibodies reflect immune feedback loop disruption, cytokine patterns indicate inflammatory loops, and norepinephrine dysregulation represents autonomic loops. Integrating molecular data with clinical and physiological assessments moves diagnosis from exclusion toward mechanistic specificity, enabling precision-targeted interventions.
5. Toward an integrated diagnostic pathway
The optimal diagnostic approach layers: (1) comprehensive clinical assessment, (2) exclusion of secondary causes, (3) autonomic testing, and (4) incorporation of biomarker or imaging data where available. This structured framework maximizes diagnostic accuracy and supports early identification of post-COVID-19 autonomic sequelae [34]. A unified model bridging bedside evaluation with emerging molecular diagnostics provides a foundation for personalized management of post-COVID-19 POTS [35].
Therapeutic approaches: multimodal resilience restoration
Management of post-COVID-19 POTS requires a multidisciplinary, phenotype-based approach, integrating lifestyle, pharmacologic, and mechanistic-targeted strategies to restore autonomic and systemic resilience [36]. Treatment follows established POTS principles, emphasizing individualized care guided by clinical phenotype, biomarker profiles, and systemic assessment.
1. Lifestyle and non-pharmacologic interventions
Key non-pharmacologic strategies target volume expansion, autonomic modulation, and mitochondrial support. Table 2 summarizes the main interventions and their mechanistic targets.
2. Pharmacologic management
Pharmacologic therapy is considered for patients with persistent debilitating symptoms, individualized according to phenotype (tachycardic, hypovolemic, hyperadrenergic). Table 3 classifies agents by mechanism and evidence strength.
3. Pathophysiology-targeted therapies
Therapies aimed at underlying mechanisms of Long COVID and POTS include:
Antiviral approaches. Persistent viral reservoirs may contribute to pathogenesis. Nirmatrelvir/ritonavir is under investigation for prolonged or personalized dosing [45].
Immunomodulatory therapies. Targeting IL-6, IL-1β, interferon, tumor necrosis factor, Janus Kinase (JAK) pathways (e.g., baricitinib, IVIG, plasmapheresis). Ongoing trials include baricitinib for neurocognitive impairment (REVERSE-LC; NCT06631287) [46].
Microbiota-targeted interventions: Gut dysbiosis influences systemic inflammation. Probiotics (e.g., Lactiplantibacillus plantarum 299v), multi-strain formulations (SIM01), and fecal microbiota transplantation are under investigation; prospective urban rural epidemiology – low-carbohydrate study (NCT06643299) examines long-term benefits [47].
Mitochondrial supportive therapies. Supplements such as antioxidants, creatine, pyrroloquinoline quinone, omega-3 fatty acids, and branched-chain amino acids support energy metabolism. Gut–mitochondria axis modulation through probiotics/prebiotics may further enhance outcomes [40].
Anticoagulation/antiplatelet therapy. Targeting microthrombosis and endothelial dysfunction. Short-term aspirin, clopidogrel, or apixaban may reduce microclot burden; therapy should be individualized based on coagulation/inflammation biomarkers [48].
4. Integrative and future directions
Management of POTS is increasingly framed as multimodal resilience restoration, addressing not only heart-rate control but systemic recalibration across autonomic, immune, endothelial, and metabolic domains [15]. Future strategies under investigation include vagal nerve stimulation, low-dose naltrexone, targeted antioxidants, and endothelial-protective agents.
Optimal outcomes emerge from multimodal synergy – combining low-dose pharmacotherapy, exercise reconditioning, cognitive-behavioral therapy, and metabolic optimization. This resilience-oriented framework holds promise for restoring adaptive homeostasis and improving long-term recovery in post-COVID-19 POTS.
A Roadmap for validation and future directions
Translating the HIM from conceptual framework to clinical utility requires a structured, multi-phase validation approach. Future research should begin with deep phenotyping and longitudinal studies tracking patients from acute infection through chronic phases, mapping the progression of systemic instability and identifying resilience biomarkers via multi-omics profiling and autonomic assessments.
Mechanistic investigations employing high-resolution physiological monitoring and computational modeling can clarify feedback loops among autonomic, immune, endothelial, and metabolic systems. Building on these insights, adaptive interventional trials should stratify patients according to their dominant instability profile – whether autoimmune, endothelial, or metabolic – and test targeted, multimodal therapies designed to restore systemic resilience. Success metrics should extend beyond symptom reduction to include objective restoration of physiological coherence across systems.
Collaborative, cross-disciplinary efforts integrating neurology, immunology, vascular biology, and systems physiology are essential to validate HIM and translate mechanistic understanding into clinical practice.
Ultimately, this work represents a systems-medicine shift – from symptom control to resilience engineering – which may redefine therapeutic goals for post-viral dysautonomia, aligning directly with the overarching theme of homeostatic instability and resilience failure.
Conclusion
Post-COVID-19 POTS illustrates how a transient viral insult can trigger chronic, systems-level failure. The HIM reframes POTS as a network pathology – an emergent collapse of interconnected autonomic, immune, endothelial, and metabolic loops – rather than a discrete autonomic defect. HIM explains why diverse findings – autoantibodies, hypovolemia, mitochondrial stress, microcirculatory dysfunction – converge into a single clinical phenotype and accounts for the relapsing, fluctuating nature of symptoms.
Therapeutically, this perspective shifts the focus from symptom suppression to resilience restoration, integrating pharmacologic modulation of adrenergic tone, endothelial protection, mitochondrial support, and neuroimmune recalibration with rehabilitation strategies encompassing autonomic retraining and metabolic conditioning.
For validation, HIM advocates a structured roadmap:
1. Quantify multi-axis instability via HRV, endothelial, immune, and metabolic biomarkers.
2. Apply network modeling to simulate recovery trajectories.
3. Conduct clinical trials assessing improvements in resilience indices rather than isolated parameters.
Operationalizing HIM through longitudinal biomarker panels and computational network mapping promises to establish a new diagnostic and therapeutic paradigm for post-viral dysautonomia.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the author
Информация об авторе
Khaled A. Abdel-Sater – MD, Prof. of Physiology, Faculty of Dentistry, Mutah University.
E-mail: Kabdelsater@mutah.edu.jo; ORCID: 0000-0001-9357-4983
Халед А. Абдель-Сатер – д-р медицины, проф. физиологии стоматологического фак-та Университета Мута. E-mail: Kabdelsater@mutah.edu.jo; ORCID: 0000-0001-9357-4983
Received: 10.10.2025
Revised: 30.10.2025
Accepted: 13.11.2025
Поступила в редакцию: 10.10.2025
Поступила после рецензирования: 30.10.2025
Принята к публикации: 13.11.2025
Список исп. литературыСкрыть список1. Narasimhan B, Calambur A, Moras E et al. Postural Orthostatic Tachycardia Syndrome in COVID-19: A Contemporary Review of Mechanisms, Clinical Course and Management. Vasc Health Risk Manag 2023;19:303-16. DOI: 10.2147/VHRM.S380270
2. Kavi L. Postural tachycardia syndrome and long COVID: an update. Br J Gen Pract 2021;72:8-9. DOI: 10.3399/bjgp22X718037
3. Taub PR, Zadourian A, Lo HC et al. Randomized trial of ivabradine in patients with hyperadrenergic postural orthostatic tachycardia syndrome. J Am Coll Cardiol 2021;77:861-71. DOI: 10.1016/j.jacc.2020.12.029
4. Hou Y, Gu T, Ni Z et al. Global prevalence of Long COVID, its subtypes, and risk factors: an updated systematic review and meta-analysis. Open Forum Infect Dis 2025;12(9):ofaf533. DOI: 10.1093/ofid/ofaf533
5. Esposito S, Puntoni M, Deolmi M et al. Long COVID in pediatric age: an observational, prospective, longitudinal, multicenter study in Italy. Front Immunol 2025;16:1466201. DOI: 10.3389/FIMMU.2025.1466201/FULL
6. Mar PL, Raj SR. Postural Orthostatic Tachycardia Syndrome: Mechanisms and New Therapies. Annu Rev Med 2020;71:235-48. DOI: 10.1146/annurev-med-041818-011630
7. Dani M, Dirksen A, Taraborrelli P et al. Autonomic dysfunction in 'long COVID': rationale, physiology and management strategies. Clin Med (Lond) 2021;21(1):e63-e67. DOI: 10.7861/clinmed.2020-0896
8. Mantovani M, Bellavite P, Fazio S et al. Autoantibodies Targeting G-Protein-Coupled Receptors and RAS-Related Molecules in Post-Acute COVID Vaccination Syndrome: A Retrospective Case Series Study. Biomedicines 2024;12(12):2852. DOI: 10.3390/biomedicines12122852
9. Alves MCS, Rego MS, Silva RCCD et al. Gut Microbiota and COVID-19: Unraveling the Gut-Lung Axis and Immunomodulatory Therapies. ACS Infect Dis 2025;11(7):1844-53. DOI: 10.1021/acsinfecdis.5c00250
10. Cornwell WK 3rd, Levine BD, Baptiste D et al. Exercise Intolerance and Response to Training in Patients With Post-acute Sequelae of SARS-CoV2 (Long COVID): A Scientific Statement From the American Heart Association. Circulation 2025;152(5):e50-e62. DOI: 10.1161/CIR.0000000000001348
11. Oba S, Hosoya T, Iwai H, Yasuda S. Long COVID: mechanisms of disease, multisystem sequelae, and prospects for treatment. Immunol Med 2025 Oct 21:1-24. DOI: 10.1080/25785826.2025.2570902
12. Shouman K, Vanichkachorn G, Cheshire WP et al. Autonomic dysfunction following COVID-19 infection: an early experience. Clin Auton Res 2021;31(3):385-94. DOI: 10.1007/s10286-021-00803-8
13. Albornoz EA, Amarilla AA, Modhiran N et al. SARS-CoV-2 drives NLRP3 inflammasome activation in human microglia through spike protein. Mol Psychiatry 2023;28(7):2878-93. DOI: 10.1038/s41380-022-01831-0
14. Yin K, Peluso MJ, Luo X et al. Long COVID manifests with T cell dysregulation, inflammation and an uncoordinated adaptive immune response to SARS-CoV-2. Nat Immunol 2024;25(2):218-25. DOI: 10.1038/s41590-023-01724-6
15. Yong SJ. Persistent brainstem dysfunction in long-COVID: a hypothesis. ACS Chem Neurosci 2021;12:573-80. DOI: 10.1021/acschemneuro.0c00793
16. Verma D, Church TM, Swaminathan S. Epstein-Barr Virus lytic replication induces ACE2 expression and enhances SARS-CoV-2 pseudotyped virus entry in epithelial cells. J Virol 2021;95(13):e0019221. DOI: 10.1128/JVI.00192-21
17. Rowntree LC, Audsley J, Allen LF et al. SARS-CoV-2-specific CD8+ T cells from people with long COVID establish and maintain effector phenotype and key TCR signatures over 2 years. Proc Natl Acad Sci U S A 2024;121(39):e2411428121. DOI: 10.1073/PNAS.2411428121
18. Santos Guedes de Sa K, Silva J, Bayarri-Olmos R et al. A causal link between autoantibodies and neurological symptoms in long COVID. medRxiv. 2024. DOI: 10.1101/2024.06.18.24309100
19. Liu Q, Mak JWY, Su Q et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut 2022;71(3):544-52. DOI: 10.1136/gutjnl-2021-325989
20. Ahmadi Badi S, Malek A, Paolini A et al. Downregulation of ACE, AGTR1, and ACE2 genes mediating SARS-CoV-2 pathogenesis by gut microbiota members and their postbiotics on Caco-2 cells. Microb Pathog 2022;173(Pt A):105798. DOI: 10.1016/j.micpath.2022.105798
21. Bourne KM, Sheldon RS, Hall J et al. Compression Garment Reduces Orthostatic Tachycardia and Symptoms in Patients With Postural Orthostatic Tachycardia Syndrome. J Am Coll Cardiol 2021;77(3):285-96. DOI: 10.1016/j.jacc.2020.11.040
22. Constantinescu-Bercu A, Kessler A, de Groot R et al. Analysis of thrombogenicity under flow reveals new insights into the prothrombotic state of patients with post-COVID syndrome. J Thromb Haemost 2023;21(1):94-100. DOI: 10.1016/j.jtha.2022.10.013
23. Guarnieri JW, Haltom JA, Albrecht YES et al. SARS-CoV-2 mitochondrial metabolic and epigenomic reprogramming in COVID-19. Pharmacol Res 2024;204:107170. DOI: 10.1016/j.phrs.2024.107170
24. Zhao S, Chen F, Yin Q et al. Reactive oxygen species interact with NLRP3 inflammasomes and are involved in the inflammation of sepsis: from mechanism to treatment of progression. Front Physiol 2020;11:571810. DOI: 10.3389/fphys.2020.571810
25. Di Florio DN, Beetler DJ, McCabe EJ et al. Mitochondrial extracellular vesicles, autoimmunity and myocarditis. Front Immunol 2024;15:1374796. DOI: 10.3389/fimmu.2024.1374796
26. Gunning WT, Khan S, Spatafore JW et al. Postural orthostatic tachycardia syndrome in post-COVID-19 long-hauler patients is associated with platelet storage pool deficiency. Front Med (Lausanne) 2025;12:1560120. DOI: 10.3389/fmed.2025.1560120
27. Rysz S, Al-Saadi J, Sjöström A et al. COVID-19 pathophysiology may be driven by an imbalance in the renin-angiotensin-aldosterone system. Nat Commun 2021;12(1):2417. DOI: 10.1038/s41467-021-22713-z
28. Fedorowski A, Fanciulli A, Raj SR et al. Cardiovascular autonomic dysfunction in post-COVID-19 syndrome: a major health-care burden. Nat Rev Cardiol 2024;21(6):379-95. DOI: 10.1038/s41569-023-00962-3
29. Mallick D, Goyal L, Chourasia P et al. COVID-19 Induced Postural Orthostatic Tachycardia Syndrome (POTS): A Review. Cureus 2023;15(3):e36955. DOI: 10.7759/cureus.36955
30. Ståhlberg M, Reistam U, Fedorowski A et al. Post-COVID-19 Tachycardia Syndrome: A Distinct Phenotype of Post-Acute COVID-19 Syndrome. Am J Med 2021;134(12):1451-6. DOI: 10.1016/j.amjmed.2021.07.004
31. Goodman BP. Evaluation of postural tachycardia syndrome (POTS). Auton Neurosci 2018;215:12-9. DOI: 10.1016/j.autneu.2018.04.004
32. Van Zanten S, Sutton R, Hamrefors V et al. Tilt table testing, methodology and practical insights for the clinic. Clin Physiol Funct Imaging 2024;44(2):119-30. DOI: 10.1111/cpf.12859
33. Pena-Hernandez C, Nugent K, Tuncel M. Twenty-Four-Hour Ambulatory Blood Pressure Monitoring. J Prim Care Community Health 2020;11:2150132720940519. DOI: 10.1177/2150132720940519
34. Tanashyan MM, Kuznetsova PI, Morozova SN et al. Neuroimaging Correlates of Post-COVID-19 Symptoms: A Functional MRI Approach. Diagnostics (Basel) 2024;14(19):2180. DOI: 10.3390/diagnostics14192180
35. Baker JR, Hira R, Uppal J, Raj SR. Clinical Assessment of the Autonomic Nervous System. Card Electrophysiol Clin 2024;16(3):239-48. DOI: 10.1016/j.ccep.2024.02.001
36. Chua EX, Zahir SMISM, Ng KT et al. Effect of prone versus supine position in COVID-19 patients: A systematic review and meta-analysis. J Clin Anesth 2021;74:110406. DOI: 10.1016/j.jclinane.2021.110406
37. Batool-Anwar S, Fashanu OS, Quan SF. Long-term Effects of COVID-19 on Sleep Patterns. Thorac Res Pract 2025;26(1):9-16. DOI: 10.5152/ThoracResPract.2024.24013
38. Snapper H, Cheshire WP. Oral and intravenous hydration in the treatment of orthostatic hypotension and postural tachycardia syndrome. Auton Neurosci 2022;238:102951. DOI: 10.1016/j.autneu.2022.102951
39. Peebles KC, Jacobs C, Makaroff L, Pacey V. The use and effectiveness of exercise for managing postural orthostatic tachycardia syndrome in young adults with joint hypermobility and related conditions: A scoping review. Auton Neurosci 2024;252:103156. DOI: 10.1016/j.autneu.2024.103156
40. Chen L-Z, Cai Q, Zheng P-F. Mitochondrial metabolic rescue in post-COVID-19 syndrome: MR spectroscopy insights and precision nutritional therapeutics. Front Immunol 2025;16:1597370. DOI: 10.3389/fimmu.2025.1597370
41. Abbate G, De Iulio B, Thomas G et al. Postural Orthostatic Tachycardia Syndrome After COVID-19: A Systematic Review of Therapeutic Interventions. J Cardiovasc Pharmacol 2023;82(1):23-31. DOI: 10.1097/FJC.0000000000001432
42. Quinn KL, Lam GY, Walsh JF et al. Cardiovascular Considerations in the Management of People With Suspected Long COVID. Can J Cardiol 2023;39(6):741-53. DOI: 10.1016/j.cjca.2023.04.003
43. Gosmann NP, Costa MA, Jaeger MB et al. Selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors for anxiety, obsessive-compulsive, and stress disorders: A 3-level network meta-analysis. PLoS Med 2021;18(6):e1003664. DOI: 10.1371/journal.pmed.1003664
44. Ormiston CK, Świątkiewicz I, Taub PR. Postural orthostatic tachycardia syndrome as a sequela of COVID-19. Heart Rhythm 2022;19(11):1880-9. DOI: 10.1016/j.hrthm.2022.07.014
45. Proal AD, Aleman S, Bomsel M et al. Targeting the SARS-CoV-2 reservoir in long COVID. Lancet Infect Dis 2025;25(5):e294-e306. DOI: 10.1016/S1473-3099(24)00769-2
46. Bronte V, Ugel S, Tinazzi E et al. Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J Clin Invest 2020;130(12):6409-16. DOI: 10.1172/JCI141772
47. Lim HX, Khalid K, Abdullah ADI et al. Subphenotypes of Long COVID and the clinical applications of probiotics. Biomed Pharmacother 2025;183:117855. DOI: 10.1016/j.biopha.2025.117855
48. Laubscher GJ, Stellenbosch M, Khan A et al. Treatment of Long COVID symptoms with triple anticoagulant therapy. Res Sq 2023. DOI: 10.21203/RS.3.RS-2697680/V1