Клинический разбор в общей медицине №05 2026
Университетская больница общего профиля им. доктора Соетомо, Сурабая, Индонезия;
Университет Айрлангга, Сурабая, Индонезия;
yunias.setiawati@fk.unair.ac.id
Аннотация
Введение. Синдром дефицита внимания и гиперактивности (СДВГ) – часто встречающееся у детей нейроонтогенетическое заболевание, характеризуемое гиперактивностью, импульсивностью и невнимательностью. Хотя медикаментозные методы, такие как терапия метилфенидатом, по-прежнему составляют основу лечения, многие дети демонстрируют недостаточный ответ на лечение или наличие нежелательных явлений, что обусловливает интерес к вспомогательным или альтернативным методам лечения. Витамин D, роль которого в развитии нервной системы и иммунной регуляции известна, недавно привлек к себе внимание из-за возможной связи с симптомами СДВГ и другими психическими заболеваниями.
Методы. В соответствии с рекомендациями PRISMA после регистрации на PROSPERO выполнены систематический обзор и метаанализ с целью оценить влияние дефицита витамина D и использования добавок с витамином D на симптомы СДВГ у детей. Проведен поиск в базах данных PubMed, ScienceDirect, а также в Cochrane Library по 28 апреля 2025 г. Были включены только рандомизированные контролируемые исследования, в которых приняли участие дети или подростки с СДВГ, получавшие добавки с витамином D или проходившие обследование по поводу дефицита витамина D. Качество исследований оценивали с помощью инструмента RoB-2, количественное обобщение выполняли с помощью Review Manager 5.4.
Результаты. Критериям включения соответствовали 6 рандомизированных контролируемых исследований, в которых приняли участие 366 человек, преимущественно из ближневосточных популяций. Анализ объединенного массива данных показал, что использование добавок с витамином D значимо улучшало общее состояние при СДВГ и облегчало симптомы гиперактивности по сравнению с контролем, при этом отсутствовало значимое влияние на когнитивные аспекты и невнимательность.
Выводы. Судя по всему, использование добавок с витамином D представляет собой безопасный и потенциально эффективный вспомогательный метод лечения, позволяющий облегчить основные симптомы СДВГ, прежде всего гиперактивность. Необходимы дальнейшие широкомасштабные многоцентровые исследования разнообразных популяций, чтобы подтвердить его лечебный эффект и уточнить стратегии выбора оптимальных доз.
Для цитирования: Ибадина З., Сетьявати Ю. Переосмысление роли витамина D в контексте синдрома дефицита внимания и гиперактивности у детей: данные систематического обзора и метаанализа. Клинический разбор в общей медицине. 2026; 7 (5): 127–132. DOI: 10.47407/kr2026.7.5.00853
Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders in children, characterized by persistent difficulties in attention, impulsivity, and hyperactivity. Its prevalence has increased over the past decades, and symptoms often continue into adolescence and adulthood, affecting learning, social adjustment, and mental health [1]. Although stimulant medications remain the mainstay of treatment, many children experience incomplete response or side effects, prompting interest in alternative or complementary interventions that are safe, affordable, and biologically plausible [2].
Nutrition has emerged as an important area of investigation in ADHD management. Several studies have explored the influence of micronutrients such as zinc, iron, and omega 3 fatty acids on cognitive and behavioral outcomes [3]. Among these, vitamin D has received increasing attention due to its role in brain function, neuroplasticity, and immune regulation. Vitamin D receptors are present in brain regions involved in attention, emotion, and executive control, suggesting a possible mechanistic link between vitamin D and ADHD [4].
Observational studies have consistently found that children with ADHD have lower serum 25 hydroxyvitamin D levels compared with healthy peers [5]. Low maternal vitamin D during pregnancy has also been associated with a higher risk of ADHD in offspring, pointing to a developmental component in this relationship [6]. Moreover, vitamin D influences neurotransmitter systems, including dopamine and serotonin pathways, and plays a regulatory role in oxidative stress and inflammation, mechanisms often implicated in ADHD pathophysiology [1].
Clinical trials have begun to test whether vitamin D supplementation can improve ADHD symptoms. A recent meta-analysis of randomized controlled trials demonstrated modest yet statistically significant improvements in total ADHD and hyperactivity scores when vitamin D was administered alongside standard therapy [4]. However, findings across studies remain inconsistent, likely due to differences in dosage, baseline deficiency, and study design.
Considering these findings, vitamin D may represent a biologically relevant and practical adjunct in managing ADHD. This systematic review and meta-analysis were conducted to synthesize current evidence on the effect of vitamin D supplementation on ADHD symptoms in children and adolescents, and to assess its clinical significance and potential role in future therapeutic strategies.
Methods
Search strategy. This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
A comprehensive literature search was conducted up to April 28, 2025, using PubMed, ScienceDirect, and the Cochrane Library. The search terms included: (“Vitamin D” OR “25(OH)D”) AND (“attention deficit hyperactivity disorder” OR “Attention deficit and hyperactivity disorder” OR “ADHD”) AND (“Supplementation” OR “Deficiency”).
Studies were screened based on titles and abstracts, and potentially relevant articles were retrieved for full-text evaluation. Eligible studies were included in both the qualitative synthesis and quantitative meta-analysis. This review was prospectively registered in PROSPERO on March 21, 2025 (registration number: CRD420251016505).
Inclusion and exclusion criteria. Studies were included if they met the following criteria:
1. Participants were children or adolescents diagnosed with ADHD.
2. The intervention involved vitamin D supplementation or assessment of vitamin D deficiency.
3. The control group received either placebo or standard therapy.
4. Outcomes included serum vitamin D levels or ADHD symptom scores after intervention.
5. The study design was a randomized controlled trial (RCT).
Exclusion criteria were:
1. Studies with unavailable full text.
2. Articles with inappropriate design, intervention, or outcome measures.
The detailed study selection process is summarized in Figure 1, following the PRISMA flow diagram.
Data extraction and quality assessment. Data were independently extracted by two reviewers and verified by a third to ensure accuracy. Extracted variables included study characteristics (author, year, country, sample size, age, intervention details, control type, dosage, and duration) and outcome measures (vitamin D serum levels and ADHD symptom scores).
Risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool, which evaluates key domains such as randomization, deviations from intended interventions, missing data, outcome measurement, and selection of reported results. Each domain was rated as low risk, some concern, or high risk. Any discrepancies were resolved through discussion until consensus was achieved.
Statistical analysis. Meta-analysis was performed using Review Manager version 5.4 (The Cochrane Collaboration, Copenhagen, Denmark). Effect sizes were expressed as standardized mean differences (SMD) with corresponding 95% confidence intervals (CI). A random-effects model was used to account for anticipated clinical heterogeneity among studies. Statistical significance was defined as p<0.05. Heterogeneity was assessed using the I² statistic, categorized as negligible (0–25%), low (26–50%), moderate (51–75%), or high (>75%). Sensitivity analyses were planned to explore sources of heterogeneity when applicable.
Results
Study selection and characteristics. A total of six randomized controlled trials met the inclusion criteria, encompassing 366 children diagnosed with ADHD across two countries: Iran and Egypt. All studies compared vitamin D supplementation with placebo in children aged 6 to 13 years, with treatment durations ranging from 6 to 12 weeks. Dosages varied from 1000 IU/day to 50,000 IU/week of cholecalciferol. The details of each study are summarized in Table 1.
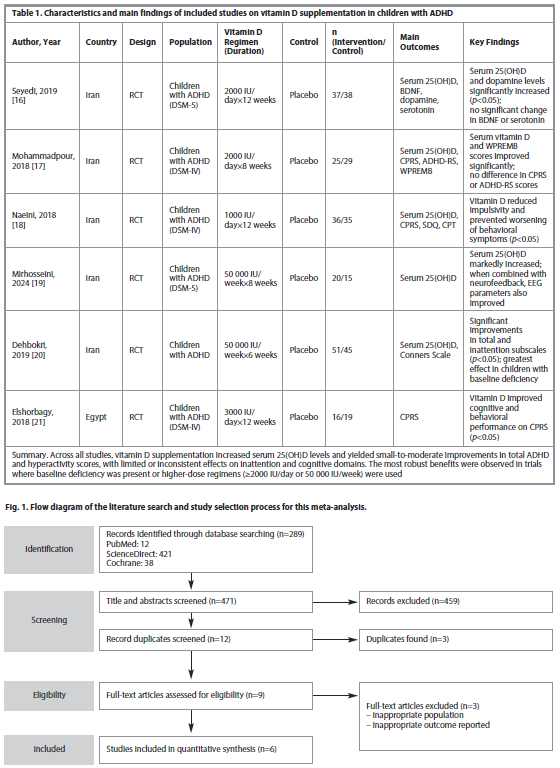
All studies utilized validated ADHD assessment tools, including the Conners’ Parent Rating Scale (CPRS), Conners’ ADHD Rating Scale (ADHD-RS), Strengths and Difficulties Questionnaire (SDQ), and Continuous Performance Test (CPT). Several studies also measured serum biomarkers such as brain-derived neurotrophic factor (BDNF), dopamine, and serotonin to evaluate potential neurobiological effects.
In most trials, vitamin D supplementation significantly increased serum 25(OH)D levels compared with placebo (p<0.05). Some studies also observed improvements in total ADHD and hyperactivity scores, while the effects on inattention and cognitive performance were less consistent.
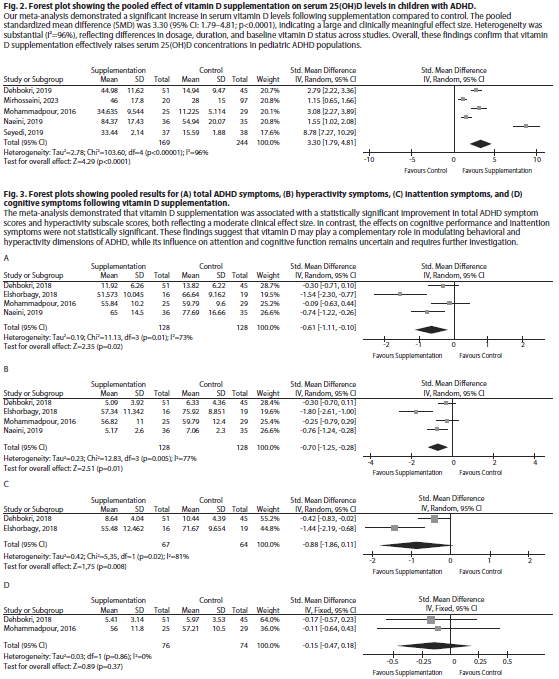
Effect of vitamin D supplementation on serum vitamin D levels. The pooled analysis demonstrated that vitamin D supplementation significantly increased serum 25(OH)D concentrations, with a standardized mean difference (SMD) of 3.30 (95% CI: 1.79–4.81; p<0.0001). Heterogeneity was high (I²=96%), reflecting differences in dosage and treatment duration across studies (Figure 2).
Effect of vitamin D on ADHD symptom scores.
A meta-analysis of symptom outcomes indicated a statistically significant reduction in total ADHD symptom scores among children receiving vitamin D supplementation compared with placebo. Improvement was most pronounced for hyperactivity symptoms, with smaller and non-significant effects observed for inattention and cognitive domains (Figure 3).
These results suggest that vitamin D supplementation can meaningfully improve certain behavioral dimensions of ADHD, particularly hyperactivity, while its effects on cognitive and attentional outcomes require further investigation.
Discussion
This meta-analysis offers new insights into the potential role of vitamin D supplementation in children with ADHD. By aggregating data from six randomized controlled trials comprising 366 participants, we confirmed that supplementation reliably raises serum 25(OH)D levels and yields modest improvements in total ADHD symptoms and hyperactivity. However, findings on inattention and cognitive domains remain equivocal. Below, we interpret these results in the context of existing literature, explore plausible biological mechanisms, highlight key caveats, and propose future directions.
Interpretation in context of prior evidence. Our findings align with earlier meta-analyses and trials suggesting a beneficial adjunctive effect of vitamin D in ADHD. For example, a pooled analysis of RCTs by [PubMed study] observed small but statistically significant improvements in total ADHD, inattention, and hyperactivity scores when vitamin D was added to methylphenidate therapy.4 Similarly, trials combining vitamin D with magnesium (50,000 IU/week + magnesium) have demonstrated improvements in behavioral and emotional outcomes in ADHD children, though not uniformly across all symptom subscales [7].
By contrast, other trials focusing on inflammatory markers found that vitamin D supplementation over three months did not significantly reduce cytokines such as IL-6 or TNF-α, despite increasing serum vitamin D levels [8]. This suggests that the behavioral improvements we observe may not be mediated solely, or even primarily, via systemic anti-inflammatory effects.
A complementary perspective comes from neurophysiological research. One study combining vitamin D supplementation and neurofeedback in children with ADHD reported not only increased serum vitamin D but favorable changes in EEG metrics, such as decreased theta-to-beta ratios and relative theta power, which correlated with improved behavioral scores [7]. These findings suggest that vitamin D might have direct effects on neural excitability or network dynamics beyond peripheral markers.
Furthermore, a recent case–control study of children with ADHD examined vitamin D status and sleep parameters. The authors found that vitamin D insufficiency was associated with worse sleep duration and greater sleep-disordered breathing, though not with direct differences in core ADHD symptom scores [9]. Because sleep disruption is known to exacerbate attention and behavioral dysregulation [10], vitamin D’s effect on ADHD might be mediated via sleep improvements in some patients.
Biological plausibility and mechanisms. Several mechanistic pathways support a potential role for vitamin D in ADHD etiology and symptom modulation:
• Neurotransmitter regulation: Vitamin D regulates enzymes and transporters involved in dopamine and serotonin pathways. It also modulates expression of tyrosine hydroxylase, a rate-limiting enzyme in dopamine synthesis [11], which is relevant to ADHD’s dopaminergic hypotheses.
• Neurotrophic and synaptic support: Vitamin D acts through its receptor (VDR) and the enzyme 1α-hydroxylase (expressed in brain) to influence gene expression related to synaptic plasticity, neuronal survival, and differentiation [12].
• Oxidative stress and neuroinflammation: In vitro and animal studies demonstrate that vitamin D downregulates pro-inflammatory cytokines, upregulates antioxidant pathways, and dampens microglial activation. These pathways are implicated in neurodevelopmental disorders and may contribute to vulnerability in ADHD.
• Neural excitability and electrophysiology: The observed EEG effects in supplemented children (e.g., shifting theta/beta ratios) hint that vitamin D may modulate neural circuit excitability or inhibit aberrant oscillatory patterns.
• Sleep regulation: Vitamin D participates in regulation of melatonin synthesis and circadian rhythm. Insufficiency may worsen sleep quality or architecture, which in turn can impair attention and executive function [13, 14], potentially amplifying ADHD symptoms.
• Developmental programming: Evidence from perinatal studies shows that higher vitamin D supplementation in infancy is associated with reduced internalizing symptoms later in childhood [15]. This suggests early vitamin D levels may have long-term neuropsychiatric effects.
These overlapping mechanisms suggest that vitamin D supplementation may exert multi-modal effects: direct modulation of brain circuits, indirect amelioration of sleep, and resilience to oxidative or inflammatory stress.
Limitations. While the findings of this meta-analysis are encouraging, several limitations should be acknowledged. All studies included in this systematic review, after screening based on the inclusion and exclusion criteria and applied methodology, were conducted in Iran and Egypt, which limits generalizability to other populations where sunlight exposure, diet, and genetic factors may differ. High heterogeneity (I²=96%) across trials reflected variation in dosage, intervention duration, and baseline vitamin D status. Most studies had small sample sizes, short follow-up periods, and moderate methodological quality, which restricts the interpretation of long-term outcomes. Moreover, vitamin D was frequently used alongside stimulant medications, making it difficult to isolate its independent effects. Despite these limitations, this analysis contributes additional evidence supporting the role of vitamin D as a potential adjunctive therapy in ADHD management and highlights the need for larger, multi-center trials across diverse populations.
Directions for future research. To advance this field meaningfully, future studies should:
• Enroll larger samples and include diverse populations across geographic, ethnic, and environmental contexts.
• Use longer follow-up periods (e.g., 6–12 months) to assess sustained response and relapse rates.
• Stratify participants by baseline vitamin D status (deficient vs sufficient) to explore differential responsiveness.
Include multi-arm designs with varying dosing regimens to identify dose-response relationships.
• Integrate mechanistic measurements such as inflammatory biomarkers, oxidative stress indices, EEG and neuroimaging, and sleep metrics (polysomnography).
• Test vitamin D monotherapy vs adjunctive therapy to assess independent effects.
• Evaluate functional outcomes (school performance, executive tests, quality of life) beyond symptom scales.
Conclusion
In sum, This meta-analysis reinforces the growing evidence that vitamin D supplementation can safely elevate serum 25(OH)D levels and may provide modest symptomatic benefits for children with ADHD, particularly in reducing total and hyperactivity scores. The findings are clinically meaningful and align with evidence linking vitamin D to neurodevelopment, neurotransmission, and immune regulation. As all included studies were conducted in Iran and Egypt, the results are most applicable to Middle Eastern populations but may also have relevance for other regions with similar sunlight exposure and dietary patterns, such as parts of Asia. Further large-scale, multicenter studies with diverse populations and longer follow-up are warranted to validate these findings and guide integration of vitamin D supplementation into clinical practice for ADHD management.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов.
Funding. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Registration/License. PROSPERO registration has been obtained for this systematic review under the following link: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD420251016505.
Contributors. All authors were involved and contributed to the conception, drafting, searching databases, review and revision of the manuscript.
Финансирование. Данное исследование не получило финансирования от каких-либо государственных, коммерческих или некоммерческих организаций.
Регистрация/лицензия. Систематический обзор был зарегистрирован на PROSPERO: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD420251016505.
Вклад авторов. Все авторы приняли участие и внесли вклад в разработку концепции, подготовку черновика рукописи, поиск в базах данных, анализ и пересмотр рукописи.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Zahra Ibadina – MD, Department of Psychiatry, Dr Soetomo General Academic Hospital; Department of Psychiatry, Faculty of Medicine – Universitas Airlangga, Surabaya, Indonesia. E-mail: zahraibadina@gmail.com; ORCID: 0009-0009-3640-0501
Захра Ибадина – д-р медицины, отд-ние психиатрии, Университетская больница общего профиля им. доктора Соетомо; каф. психиатрии, медицинский факультет, Университет Айрлангга, Сурабая, Индонезия. E-mail: zahraibadina@gmail.com; ORCID: 0009-0009-3640-0501
Yunias Setiawati – MD, PhD, Prof., Department of Psychiatry, Dr Soetomo General Academic Hospital; Department of Psychiatry, Faculty of Medicine – Universitas Airlangga, Surabaya, Indonesia. E-mail: yunias.setiawati@fk.unair.ac.id; ORCID: 0000-0002-5920-3676; Scopus ID: 57211331105
Юниас Сетьявати – д-р медицины, PhD, проф., отд-ние психиатрии, Университетская больница общего профиля им. доктора Соетомо; каф. психиатрии, медицинский факультет, Университет Айрлангга, Сурабая, Индонезия. E-mail: yunias.setiawati@fk.unair.ac.id; ORCID: 0000-0002-5920-3676; Scopus ID: 57211331105
Received: 02.12.2025
Revised: 10.12.2025
Accepted: 18.12.2025
Поступила в редакцию: 02.12.2025
Поступила после рецензирования: 10.12.2025
Принята к публикации: 18.12.2025
Клинический разбор в общей медицине №05 2026
Revisiting vitamin D in pediatric attention deficit hyperactivity disorder: evidence from a systematic review and meta-analysis
Номера страниц в выпуске:127-132
Abstract
Introduction. Attention deficit hyperactivity disorder (ADHD) is a prevalent neurodevelopmental disorder in children, characterized by hyperactivity, impulsivity, and inattention. Although pharmacological treatments such as methylphenidate remain the mainstay of therapy, many children either respond inadequately or experience adverse effects, prompting interest in adjunctive or alternative interventions. Vitamin D, known for its role in neurodevelopment and immune regulation, has recently attracted attention due to its potential link with ADHD symptoms and other psychiatric conditions.
Methods. Following PRISMA guidelines and registered with PROSPERO, a systematic review and meta-analysis were conducted to evaluate the effects of vitamin D deficiency and supplementation on ADHD symptoms in children. Databases searched included PubMed, ScienceDirect, and the Cochrane Library through April 28, 2025. Only randomized controlled trials (RCTs) involving children or adolescents with ADHD receiving vitamin D supplementation or assessed for deficiency were included. Study quality was appraised using the RoB-2 tool, and quantitative synthesis was performed using Review Manager 5.4.
Results. Six RCTs comprising 366 participants, predominantly from Middle Eastern populations, met the inclusion criteria. Pooled analysis demonstrated that vitamin D supplementation significantly improved total ADHD scores and hyperactivity symptoms compared to controls, though no significant effects were observed on cognitive or inattention domains.
Conclusion. Vitamin D supplementation appears to be a safe and potentially effective adjunctive therapy for improving core ADHD symptoms, particularly hyperactivity. Further large-scale, multicenter studies across diverse populations are warranted to confirm its therapeutic role and clarify optimal dosing strategies.
For citation: Ibadina Z., Setiawati Yu. Revisiting vitamin D in pediatric attention deficit hyperactivity disorder: evidence from a systematic review and meta-analysis. Clinical review for general practice. 2026; 7 (5): 127–132 (In Russ.). DOI: 10.47407/kr2026.7.5.00853
Introduction. Attention deficit hyperactivity disorder (ADHD) is a prevalent neurodevelopmental disorder in children, characterized by hyperactivity, impulsivity, and inattention. Although pharmacological treatments such as methylphenidate remain the mainstay of therapy, many children either respond inadequately or experience adverse effects, prompting interest in adjunctive or alternative interventions. Vitamin D, known for its role in neurodevelopment and immune regulation, has recently attracted attention due to its potential link with ADHD symptoms and other psychiatric conditions.
Methods. Following PRISMA guidelines and registered with PROSPERO, a systematic review and meta-analysis were conducted to evaluate the effects of vitamin D deficiency and supplementation on ADHD symptoms in children. Databases searched included PubMed, ScienceDirect, and the Cochrane Library through April 28, 2025. Only randomized controlled trials (RCTs) involving children or adolescents with ADHD receiving vitamin D supplementation or assessed for deficiency were included. Study quality was appraised using the RoB-2 tool, and quantitative synthesis was performed using Review Manager 5.4.
Results. Six RCTs comprising 366 participants, predominantly from Middle Eastern populations, met the inclusion criteria. Pooled analysis demonstrated that vitamin D supplementation significantly improved total ADHD scores and hyperactivity symptoms compared to controls, though no significant effects were observed on cognitive or inattention domains.
Conclusion. Vitamin D supplementation appears to be a safe and potentially effective adjunctive therapy for improving core ADHD symptoms, particularly hyperactivity. Further large-scale, multicenter studies across diverse populations are warranted to confirm its therapeutic role and clarify optimal dosing strategies.
For citation: Ibadina Z., Setiawati Yu. Revisiting vitamin D in pediatric attention deficit hyperactivity disorder: evidence from a systematic review and meta-analysis. Clinical review for general practice. 2026; 7 (5): 127–132 (In Russ.). DOI: 10.47407/kr2026.7.5.00853
Переосмысление роли витамина D в контексте синдрома дефицита внимания и гиперактивности у детей: данные систематического обзора и метаанализа
З. Ибадина, Ю. СетьяватиУниверситетская больница общего профиля им. доктора Соетомо, Сурабая, Индонезия;
Университет Айрлангга, Сурабая, Индонезия;
yunias.setiawati@fk.unair.ac.id
Аннотация
Введение. Синдром дефицита внимания и гиперактивности (СДВГ) – часто встречающееся у детей нейроонтогенетическое заболевание, характеризуемое гиперактивностью, импульсивностью и невнимательностью. Хотя медикаментозные методы, такие как терапия метилфенидатом, по-прежнему составляют основу лечения, многие дети демонстрируют недостаточный ответ на лечение или наличие нежелательных явлений, что обусловливает интерес к вспомогательным или альтернативным методам лечения. Витамин D, роль которого в развитии нервной системы и иммунной регуляции известна, недавно привлек к себе внимание из-за возможной связи с симптомами СДВГ и другими психическими заболеваниями.
Методы. В соответствии с рекомендациями PRISMA после регистрации на PROSPERO выполнены систематический обзор и метаанализ с целью оценить влияние дефицита витамина D и использования добавок с витамином D на симптомы СДВГ у детей. Проведен поиск в базах данных PubMed, ScienceDirect, а также в Cochrane Library по 28 апреля 2025 г. Были включены только рандомизированные контролируемые исследования, в которых приняли участие дети или подростки с СДВГ, получавшие добавки с витамином D или проходившие обследование по поводу дефицита витамина D. Качество исследований оценивали с помощью инструмента RoB-2, количественное обобщение выполняли с помощью Review Manager 5.4.
Результаты. Критериям включения соответствовали 6 рандомизированных контролируемых исследований, в которых приняли участие 366 человек, преимущественно из ближневосточных популяций. Анализ объединенного массива данных показал, что использование добавок с витамином D значимо улучшало общее состояние при СДВГ и облегчало симптомы гиперактивности по сравнению с контролем, при этом отсутствовало значимое влияние на когнитивные аспекты и невнимательность.
Выводы. Судя по всему, использование добавок с витамином D представляет собой безопасный и потенциально эффективный вспомогательный метод лечения, позволяющий облегчить основные симптомы СДВГ, прежде всего гиперактивность. Необходимы дальнейшие широкомасштабные многоцентровые исследования разнообразных популяций, чтобы подтвердить его лечебный эффект и уточнить стратегии выбора оптимальных доз.
Для цитирования: Ибадина З., Сетьявати Ю. Переосмысление роли витамина D в контексте синдрома дефицита внимания и гиперактивности у детей: данные систематического обзора и метаанализа. Клинический разбор в общей медицине. 2026; 7 (5): 127–132. DOI: 10.47407/kr2026.7.5.00853
Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders in children, characterized by persistent difficulties in attention, impulsivity, and hyperactivity. Its prevalence has increased over the past decades, and symptoms often continue into adolescence and adulthood, affecting learning, social adjustment, and mental health [1]. Although stimulant medications remain the mainstay of treatment, many children experience incomplete response or side effects, prompting interest in alternative or complementary interventions that are safe, affordable, and biologically plausible [2].
Nutrition has emerged as an important area of investigation in ADHD management. Several studies have explored the influence of micronutrients such as zinc, iron, and omega 3 fatty acids on cognitive and behavioral outcomes [3]. Among these, vitamin D has received increasing attention due to its role in brain function, neuroplasticity, and immune regulation. Vitamin D receptors are present in brain regions involved in attention, emotion, and executive control, suggesting a possible mechanistic link between vitamin D and ADHD [4].
Observational studies have consistently found that children with ADHD have lower serum 25 hydroxyvitamin D levels compared with healthy peers [5]. Low maternal vitamin D during pregnancy has also been associated with a higher risk of ADHD in offspring, pointing to a developmental component in this relationship [6]. Moreover, vitamin D influences neurotransmitter systems, including dopamine and serotonin pathways, and plays a regulatory role in oxidative stress and inflammation, mechanisms often implicated in ADHD pathophysiology [1].
Clinical trials have begun to test whether vitamin D supplementation can improve ADHD symptoms. A recent meta-analysis of randomized controlled trials demonstrated modest yet statistically significant improvements in total ADHD and hyperactivity scores when vitamin D was administered alongside standard therapy [4]. However, findings across studies remain inconsistent, likely due to differences in dosage, baseline deficiency, and study design.
Considering these findings, vitamin D may represent a biologically relevant and practical adjunct in managing ADHD. This systematic review and meta-analysis were conducted to synthesize current evidence on the effect of vitamin D supplementation on ADHD symptoms in children and adolescents, and to assess its clinical significance and potential role in future therapeutic strategies.
Methods
Search strategy. This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
A comprehensive literature search was conducted up to April 28, 2025, using PubMed, ScienceDirect, and the Cochrane Library. The search terms included: (“Vitamin D” OR “25(OH)D”) AND (“attention deficit hyperactivity disorder” OR “Attention deficit and hyperactivity disorder” OR “ADHD”) AND (“Supplementation” OR “Deficiency”).
Studies were screened based on titles and abstracts, and potentially relevant articles were retrieved for full-text evaluation. Eligible studies were included in both the qualitative synthesis and quantitative meta-analysis. This review was prospectively registered in PROSPERO on March 21, 2025 (registration number: CRD420251016505).
Inclusion and exclusion criteria. Studies were included if they met the following criteria:
1. Participants were children or adolescents diagnosed with ADHD.
2. The intervention involved vitamin D supplementation or assessment of vitamin D deficiency.
3. The control group received either placebo or standard therapy.
4. Outcomes included serum vitamin D levels or ADHD symptom scores after intervention.
5. The study design was a randomized controlled trial (RCT).
Exclusion criteria were:
1. Studies with unavailable full text.
2. Articles with inappropriate design, intervention, or outcome measures.
The detailed study selection process is summarized in Figure 1, following the PRISMA flow diagram.
Data extraction and quality assessment. Data were independently extracted by two reviewers and verified by a third to ensure accuracy. Extracted variables included study characteristics (author, year, country, sample size, age, intervention details, control type, dosage, and duration) and outcome measures (vitamin D serum levels and ADHD symptom scores).
Risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool, which evaluates key domains such as randomization, deviations from intended interventions, missing data, outcome measurement, and selection of reported results. Each domain was rated as low risk, some concern, or high risk. Any discrepancies were resolved through discussion until consensus was achieved.
Statistical analysis. Meta-analysis was performed using Review Manager version 5.4 (The Cochrane Collaboration, Copenhagen, Denmark). Effect sizes were expressed as standardized mean differences (SMD) with corresponding 95% confidence intervals (CI). A random-effects model was used to account for anticipated clinical heterogeneity among studies. Statistical significance was defined as p<0.05. Heterogeneity was assessed using the I² statistic, categorized as negligible (0–25%), low (26–50%), moderate (51–75%), or high (>75%). Sensitivity analyses were planned to explore sources of heterogeneity when applicable.
Results
Study selection and characteristics. A total of six randomized controlled trials met the inclusion criteria, encompassing 366 children diagnosed with ADHD across two countries: Iran and Egypt. All studies compared vitamin D supplementation with placebo in children aged 6 to 13 years, with treatment durations ranging from 6 to 12 weeks. Dosages varied from 1000 IU/day to 50,000 IU/week of cholecalciferol. The details of each study are summarized in Table 1.
All studies utilized validated ADHD assessment tools, including the Conners’ Parent Rating Scale (CPRS), Conners’ ADHD Rating Scale (ADHD-RS), Strengths and Difficulties Questionnaire (SDQ), and Continuous Performance Test (CPT). Several studies also measured serum biomarkers such as brain-derived neurotrophic factor (BDNF), dopamine, and serotonin to evaluate potential neurobiological effects.
In most trials, vitamin D supplementation significantly increased serum 25(OH)D levels compared with placebo (p<0.05). Some studies also observed improvements in total ADHD and hyperactivity scores, while the effects on inattention and cognitive performance were less consistent.
Effect of vitamin D supplementation on serum vitamin D levels. The pooled analysis demonstrated that vitamin D supplementation significantly increased serum 25(OH)D concentrations, with a standardized mean difference (SMD) of 3.30 (95% CI: 1.79–4.81; p<0.0001). Heterogeneity was high (I²=96%), reflecting differences in dosage and treatment duration across studies (Figure 2).
Effect of vitamin D on ADHD symptom scores.
A meta-analysis of symptom outcomes indicated a statistically significant reduction in total ADHD symptom scores among children receiving vitamin D supplementation compared with placebo. Improvement was most pronounced for hyperactivity symptoms, with smaller and non-significant effects observed for inattention and cognitive domains (Figure 3).
These results suggest that vitamin D supplementation can meaningfully improve certain behavioral dimensions of ADHD, particularly hyperactivity, while its effects on cognitive and attentional outcomes require further investigation.
Discussion
This meta-analysis offers new insights into the potential role of vitamin D supplementation in children with ADHD. By aggregating data from six randomized controlled trials comprising 366 participants, we confirmed that supplementation reliably raises serum 25(OH)D levels and yields modest improvements in total ADHD symptoms and hyperactivity. However, findings on inattention and cognitive domains remain equivocal. Below, we interpret these results in the context of existing literature, explore plausible biological mechanisms, highlight key caveats, and propose future directions.
Interpretation in context of prior evidence. Our findings align with earlier meta-analyses and trials suggesting a beneficial adjunctive effect of vitamin D in ADHD. For example, a pooled analysis of RCTs by [PubMed study] observed small but statistically significant improvements in total ADHD, inattention, and hyperactivity scores when vitamin D was added to methylphenidate therapy.4 Similarly, trials combining vitamin D with magnesium (50,000 IU/week + magnesium) have demonstrated improvements in behavioral and emotional outcomes in ADHD children, though not uniformly across all symptom subscales [7].
By contrast, other trials focusing on inflammatory markers found that vitamin D supplementation over three months did not significantly reduce cytokines such as IL-6 or TNF-α, despite increasing serum vitamin D levels [8]. This suggests that the behavioral improvements we observe may not be mediated solely, or even primarily, via systemic anti-inflammatory effects.
A complementary perspective comes from neurophysiological research. One study combining vitamin D supplementation and neurofeedback in children with ADHD reported not only increased serum vitamin D but favorable changes in EEG metrics, such as decreased theta-to-beta ratios and relative theta power, which correlated with improved behavioral scores [7]. These findings suggest that vitamin D might have direct effects on neural excitability or network dynamics beyond peripheral markers.
Furthermore, a recent case–control study of children with ADHD examined vitamin D status and sleep parameters. The authors found that vitamin D insufficiency was associated with worse sleep duration and greater sleep-disordered breathing, though not with direct differences in core ADHD symptom scores [9]. Because sleep disruption is known to exacerbate attention and behavioral dysregulation [10], vitamin D’s effect on ADHD might be mediated via sleep improvements in some patients.
Biological plausibility and mechanisms. Several mechanistic pathways support a potential role for vitamin D in ADHD etiology and symptom modulation:
• Neurotransmitter regulation: Vitamin D regulates enzymes and transporters involved in dopamine and serotonin pathways. It also modulates expression of tyrosine hydroxylase, a rate-limiting enzyme in dopamine synthesis [11], which is relevant to ADHD’s dopaminergic hypotheses.
• Neurotrophic and synaptic support: Vitamin D acts through its receptor (VDR) and the enzyme 1α-hydroxylase (expressed in brain) to influence gene expression related to synaptic plasticity, neuronal survival, and differentiation [12].
• Oxidative stress and neuroinflammation: In vitro and animal studies demonstrate that vitamin D downregulates pro-inflammatory cytokines, upregulates antioxidant pathways, and dampens microglial activation. These pathways are implicated in neurodevelopmental disorders and may contribute to vulnerability in ADHD.
• Neural excitability and electrophysiology: The observed EEG effects in supplemented children (e.g., shifting theta/beta ratios) hint that vitamin D may modulate neural circuit excitability or inhibit aberrant oscillatory patterns.
• Sleep regulation: Vitamin D participates in regulation of melatonin synthesis and circadian rhythm. Insufficiency may worsen sleep quality or architecture, which in turn can impair attention and executive function [13, 14], potentially amplifying ADHD symptoms.
• Developmental programming: Evidence from perinatal studies shows that higher vitamin D supplementation in infancy is associated with reduced internalizing symptoms later in childhood [15]. This suggests early vitamin D levels may have long-term neuropsychiatric effects.
These overlapping mechanisms suggest that vitamin D supplementation may exert multi-modal effects: direct modulation of brain circuits, indirect amelioration of sleep, and resilience to oxidative or inflammatory stress.
Limitations. While the findings of this meta-analysis are encouraging, several limitations should be acknowledged. All studies included in this systematic review, after screening based on the inclusion and exclusion criteria and applied methodology, were conducted in Iran and Egypt, which limits generalizability to other populations where sunlight exposure, diet, and genetic factors may differ. High heterogeneity (I²=96%) across trials reflected variation in dosage, intervention duration, and baseline vitamin D status. Most studies had small sample sizes, short follow-up periods, and moderate methodological quality, which restricts the interpretation of long-term outcomes. Moreover, vitamin D was frequently used alongside stimulant medications, making it difficult to isolate its independent effects. Despite these limitations, this analysis contributes additional evidence supporting the role of vitamin D as a potential adjunctive therapy in ADHD management and highlights the need for larger, multi-center trials across diverse populations.
Directions for future research. To advance this field meaningfully, future studies should:
• Enroll larger samples and include diverse populations across geographic, ethnic, and environmental contexts.
• Use longer follow-up periods (e.g., 6–12 months) to assess sustained response and relapse rates.
• Stratify participants by baseline vitamin D status (deficient vs sufficient) to explore differential responsiveness.
Include multi-arm designs with varying dosing regimens to identify dose-response relationships.
• Integrate mechanistic measurements such as inflammatory biomarkers, oxidative stress indices, EEG and neuroimaging, and sleep metrics (polysomnography).
• Test vitamin D monotherapy vs adjunctive therapy to assess independent effects.
• Evaluate functional outcomes (school performance, executive tests, quality of life) beyond symptom scales.
Conclusion
In sum, This meta-analysis reinforces the growing evidence that vitamin D supplementation can safely elevate serum 25(OH)D levels and may provide modest symptomatic benefits for children with ADHD, particularly in reducing total and hyperactivity scores. The findings are clinically meaningful and align with evidence linking vitamin D to neurodevelopment, neurotransmission, and immune regulation. As all included studies were conducted in Iran and Egypt, the results are most applicable to Middle Eastern populations but may also have relevance for other regions with similar sunlight exposure and dietary patterns, such as parts of Asia. Further large-scale, multicenter studies with diverse populations and longer follow-up are warranted to validate these findings and guide integration of vitamin D supplementation into clinical practice for ADHD management.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов.
Funding. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Registration/License. PROSPERO registration has been obtained for this systematic review under the following link: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD420251016505.
Contributors. All authors were involved and contributed to the conception, drafting, searching databases, review and revision of the manuscript.
Финансирование. Данное исследование не получило финансирования от каких-либо государственных, коммерческих или некоммерческих организаций.
Регистрация/лицензия. Систематический обзор был зарегистрирован на PROSPERO: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD420251016505.
Вклад авторов. Все авторы приняли участие и внесли вклад в разработку концепции, подготовку черновика рукописи, поиск в базах данных, анализ и пересмотр рукописи.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Zahra Ibadina – MD, Department of Psychiatry, Dr Soetomo General Academic Hospital; Department of Psychiatry, Faculty of Medicine – Universitas Airlangga, Surabaya, Indonesia. E-mail: zahraibadina@gmail.com; ORCID: 0009-0009-3640-0501
Захра Ибадина – д-р медицины, отд-ние психиатрии, Университетская больница общего профиля им. доктора Соетомо; каф. психиатрии, медицинский факультет, Университет Айрлангга, Сурабая, Индонезия. E-mail: zahraibadina@gmail.com; ORCID: 0009-0009-3640-0501
Yunias Setiawati – MD, PhD, Prof., Department of Psychiatry, Dr Soetomo General Academic Hospital; Department of Psychiatry, Faculty of Medicine – Universitas Airlangga, Surabaya, Indonesia. E-mail: yunias.setiawati@fk.unair.ac.id; ORCID: 0000-0002-5920-3676; Scopus ID: 57211331105
Юниас Сетьявати – д-р медицины, PhD, проф., отд-ние психиатрии, Университетская больница общего профиля им. доктора Соетомо; каф. психиатрии, медицинский факультет, Университет Айрлангга, Сурабая, Индонезия. E-mail: yunias.setiawati@fk.unair.ac.id; ORCID: 0000-0002-5920-3676; Scopus ID: 57211331105
Received: 02.12.2025
Revised: 10.12.2025
Accepted: 18.12.2025
Поступила в редакцию: 02.12.2025
Поступила после рецензирования: 10.12.2025
Принята к публикации: 18.12.2025
Список исп. литературыСкрыть список1. Faraone SV, Bellgrove MA, Brikell I et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers 2024;10(1):11.
2. Nanda A, Janga LSN, Sambe HG et al. Adverse Effects of Stimulant Interventions for Attention Deficit Hyperactivity Disorder (ADHD): A Comprehensive Systematic Review. Cureus 2023;15(9):e45995.
3. Lange KW. Micronutrients and Diets in the Treatment of Attention-Deficit/Hyperactivity Disorder: Chances and Pitfalls. Front Psychiatry 2020;11:102.
4. Gan J, Galer P, Ma D et al. The Effect of Vitamin D Supplementation on Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Child Adolesc Psychopharmacol 2019;29(9):670-87.
5. Yang J, Yuan H, Qiu R, Fu X. Effect of 25 hydroxyvitamin D on attention deficit and hyperactivity in school-age children with ADHD. Medicine (Baltimore) 2023;102(43):e35728.
6. Sucksdorff M, Brown AS, Chudal R et al. Maternal Vitamin D Levels and the Risk of Offspring Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry 2021;60(1):142-151.e2.
7. Hemamy M, Pahlavani N, Amanollahi A et al. The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr 2021;21(1):178.
8. Samadi M, Gholami F, Seyedi M et al. Effect of Vitamin D Supplementation on Inflammatory Biomarkers in School-Aged Children with Attention Deficit Hyperactivity Disorder. Int J Clin Pract 2022;2022:1256408.
9. Zhang P, Liu Y, Ma Y et al. Vitamin D insufficiency and sleep disturbances in children with ADHD: a case-control study. Front Psychiatry 2025;16:1546692.
10. Hyndych A, El-Abassi R, Mader EC Jr. The Role of Sleep and the Effects of Sleep Loss on Cognitive, Affective, and Behavioral Processes. Cureus 2025;17(5):e84232.
11. Cui X, Pertile R, Liu P, Eyles DW. Vitamin D regulates tyrosine hydroxylase expression: N-cadherin a possible mediator. Neuroscience 2015;304:90-100.
12. Lv L, Tan X, Peng X et al. The relationships of vitamin D, vitamin D receptor gene polymorphisms, and vitamin D supplementation with Parkinson's disease. Transl Neurodegener 2020;9(1):34.
13. Mirarchi A, Albi E, Beccari T, Arcuri C. Microglia and Brain Disorders: The Role of Vitamin D and Its Receptor. Int J Mol Sci 2023;24(15):11892.
14. Calvello R, Cianciulli A, Nicolardi G et al. Vitamin D Treatment Attenuates Neuroinflammation and Dopaminergic Neurodegeneration in an Animal Model of Parkinson's Disease, Shifting M1 to M2 Microglia Responses. J Neuroimmune Pharmacol 2017;12(2):327-339.
15. Sandboge S, Räikkönen K, Lahti-Pulkkinen M et al. Effect of Vitamin D3 Supplementation in the First 2 Years of Life on Psychiatric Symptoms at Ages 6 to 8 Years: A Randomized Clinical Trial. JAMA Netw Open 2023;6(5):e2314319.
16. Seyedi M, Gholami F, Samadi M et al. The Effect of Vitamin D3 Supplementation on Serum BDNF, Dopamine, and Serotonin in Children with Attention-Deficit/Hyperactivity Disorder. CNS Neurol Disord Drug Targets 2019;18(6):496-501.
17. Mohammadpour N, Jazayeri S, Tehrani-Doost M et al. Effect of vitamin D supplementation as adjunctive therapy to methylphenidate on ADHD symptoms: A randomized, double blind, placebo-controlled trial. Nutr Neurosci 2018;21(3):202-9.
18. Naeini AA, Fasihi F, Najafi M et al. The effects of vitamin D supplementation on ADHD (Attention Deficit Hyperactivity Disorder) in 6–13 year-old students: A randomized, double-blind, placebo-controlled study. Eur J Integrative Med 2018;25:28-33.
19. Mirhosseini H, Maayeshi N, Hooshmandi H et al. The effect of vitamin D supplementation on the brain mapping and behavioral performance of children with ADHD: a double-blinded randomized controlled trials. Nutr Neurosci 2024;27(6):566-76.
20. Dehbokri N, Noorazar G, Ghaffari A et al. Effect of vitamin D treatment in children with attention-deficit hyperactivity disorder. World J Pediatr 2019;15(1):78-84.
21. Elshorbagy HH, Barseem NF, Abdelghani WE et al. Impact of Vitamin D Supplementation on Attention-Deficit Hyperactivity Disorder in Children. Ann Pharmacother 2018;52(7):623-631.