Клинический разбор в общей медицине №06 2026
Арбинд Кумар Чоудхари4
1 Многопрофильная больница Лакшамана, Пикара, Мадурай, Индия;
2 Медицинский колледж Американского университета Антигуа, Сент-Джонс, Антигуа и Барбуда;
3 Университетский колледж Манипал, Малайзия;
4 Государственный медицинский колледж и больница Ироду, Тамилнад, Индия
arbindkch@gmail.com
Аннотация
Агонисты рецепторов глюкагоноподобного пептида-1 (аГПП-1) стремительно меняют подходы к лечению метаболических и сердечно-сосудистых заболеваний, и теперь их используют не только при сахарном диабете 2-го типа, но и при ожирении, для защиты сердечно-сосудистой системы, при стеатозе печени и в качестве потенциальных нейропротекторов. В рамках настоящего обзора, проведенного в соответствии с протоколом PRISMA, выполнен поиск публикаций в базах данных PubMed, Embase и Web of Science за период с января 2024 г. по ноябрь 2025 г. Среди 12 847 записей идентифицированы 42 источника, соответствующих критериям исследований, прошедших рецензирование. В ходе исследований аГПП-1 снижали уровень HbA1c примерно на 0,5–2,4%, приводили к снижению массы тела на 1–25 кг и уменьшали количество серьезных неблагоприятных сердечно-сосудистых событий на 12–26%. Новые данные указывают на значительные преимущества, выходящие за рамки контроля уровня глюкозы в крови, такие как снижение риска развития деменции, улучшение исходов лечения сердечной недостаточности с сохраненной фракцией выброса и заметное уменьшение стеатоза печени при применении новых двойных и тройных агонистов. Симптомы со стороны желудочно-кишечного тракта часто встречались, но обычно их можно было контролировать путем тщательного подбора дозы и применения поддерживающих мер. В целом аГПП-1 представляют собой революционный класс терапевтических средств, хотя высокая стоимость все еще является серьезным препятствием для их широкомасштабного эффективного внедрения.
Ключевые слова: агонисты рецепторов глюкагоноподобного пептида-1, обзор, сахарный диабет 2-го типа, ожирение, сердечно-сосудистые осложнения, болезнь печени, нейропротекция, экономическая эффективность.
Для цитирования: Харини Мутурадж, Шьямала Ганесан, Мадхан Кумар Соуталлу Джанакирам, Арбинд Кумар Чоудхари. Препараты на основе агонистов рецепторов ГПП-1: комплексный обзор механизмов действия, эффективности, безопасности и новых способов применения при метаболических и сердечно-сосудистых заболеваниях. Клинический разбор в общей медицине. 2026; 7 (6): 22–28. DOI: 10.47407/kr2026.7.6.00858
Introduction
Over the past decade, glucagon-like peptide-1 receptor agonists (GLP-1RAs) have profoundly transformed the management of metabolic and cardiovascular diseases. Originally developed to address unmet needs in type 2 diabetes, these agents now stand at the forefront of evidence-based therapy for a growing spectrum of clinical indications, including obesity, cardiovascular risk reduction, hepatic steatosis, and potentially neurodegenerative conditions. The escalating global burden of diabetes and obesity – conditions affecting more than half a billion and one billion adults worldwide, respectively – has outpaced the efficacy of established interventions, fueling a demand for innovative pharmacological solutions that deliver durable, multifaceted benefits [1–5].
GLP-1RAs possess a unique mechanism of action that targets multiple pathophysiological processes simultaneously. By enhancing glucose-dependent insulin secretion, suppressing glucagon release, delaying gastric emptying, and acting centrally to reduce appetite, these agents offer pleiotropic effects that extend well beyond glycemic control. Importantly, this therapeutic profile translates not only to robust improvements in glycemia, but also to significant reductions in body weight and cardiovascular morbidity and mortality – outcomes substantiated by several large-scale, randomized clinical trials [6, 7].
In the past five years, the clinical landscape has rapidly evolved with the advent of next-generation agents, including dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) agonists and triple agonists that further amplify metabolic, hepatic, and cardiorenal benefits [8, 9]. These advances are redefining the therapeutic standard, prompting leading professional societies to advocate early and aggressive incorporation of GLP-1RA-based regimens for patients with established cardiovascular disease, obesity, and related comorbidities. Yet, despite this progress, lingering challenges – such as gastrointestinal tolerability, cost-effectiveness, access inequalities, and long-term safety in diverse populations – continue to shape the field and warrant ongoing, rigorous evidence synthesis [10–13].
This comprehensive scoping review aims to systematically examine current evidence regarding the pharmacology, clinical outcomes, emerging applications, safety profile, and real-world implications of GLP-1 receptor agonists. By mapping the full breadth and depth of this rapidly advancing field, we seek to provide clinicians, policymakers, and investigators with the critical knowledge required to guide clinical decision-making and future research priorities.
Methods
Study design and methodology framework. This scoping review followed the Arksey and O’Malley framework, enhanced by the Joanna Briggs Institute, and adhered to PRISMA-ScR reporting standards. Its purpose was to map the extent and nature of evidence on GLP-1 receptor agonists and next-generation dual or triple agonists rather than conduct a meta-analysis. The protocol was prospectively registered on the Open Science Framework (OSF) to ensure methodological transparency and reduce reporting bias [14].
Research question and objectives. The review addressed the question: What does contemporary literature reveal about mechanisms, pharmacokinetics, clinical efficacy, safety, emerging indications, and economic considerations of GLP-1 receptor agonists and related agents? Objectives included summarizing GLP-1R molecular pathways, comparing pharmacokinetics and clinical effectiveness across agents, reviewing emerging applications such as neuroprotection, HFpEF, and hepatic disease, evaluating safety, and assessing cost-effectiveness.
Eligibility criteria. Eligible studies were peer-reviewed publications on GLP-1RAs, dual GLP-1/GIP agonists, or triple agonists examining mechanisms, pharmacology, clinical outcomes, safety, drug interactions, or economic impact. Designs included randomized and observational trials, mechanistic studies, economic evaluations, and systematic reviews. Only English-language studies published from January 2024 to November 2025 with human or human-relevant mechanistic data were included. Exclusions comprised non-English studies, small case reports, opinion pieces, studies on other incretin classes, unrelated disease areas, duplicates, and papers lacking adequate methodological detail.
 Information sources and search strategy. Searches of PubMed, Embase, Web of Science, Cochrane Central, and Google Scholar identified 12,847 records. Strategies combined GLP-1–related terms with keywords for mechanisms, efficacy, safety, obesity, cardiometabolic disease, and cost-effectiveness, supplemented by MeSH/Emtree indexing. Grey literature sources included ClinicalTrials.gov, reference lists, and major society conference proceedings.
Information sources and search strategy. Searches of PubMed, Embase, Web of Science, Cochrane Central, and Google Scholar identified 12,847 records. Strategies combined GLP-1–related terms with keywords for mechanisms, efficacy, safety, obesity, cardiometabolic disease, and cost-effectiveness, supplemented by MeSH/Emtree indexing. Grey literature sources included ClinicalTrials.gov, reference lists, and major society conference proceedings.
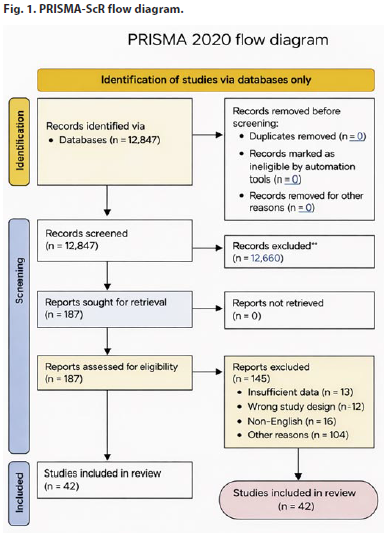
Study Selection process. All records were screened in Covidence. Two reviewers independently assessed titles and abstracts (kappa 0.92). Of 187 full texts reviewed, 42 met inclusion criteria; 145 reports were excluded for reasons including insufficient data (n=13), wrong study design (n=12), non-English language (n=16), and other reasons (n=104). The selection process is summarized in a PRISMA-ScR flow diagram (fig. 1).
Data extraction and charting. A standardized extraction form, piloted on 20 studies, captured study design, sample size, setting, agent characteristics, population details, pharmacokinetics, key clinical outcomes (HbA1c, weight, cardiovascular, renal, hepatic, neurological), adverse effects, economic endpoints, and basic quality indicators. Two reviewers extracted data independently; discrepancies (~3.2%) were resolved by discussion or source verification.
Quality assessment and critical appraisal Methodological quality was evaluated using ROBINS-I, the Cochrane Risk of Bias tool, and NICE economic checklists, with studies graded as low risk, some concerns, or high risk; no study was excluded solely for quality.
Data Synthesis and Analysis Data were narratively synthesized by thematic domains, with quantitative findings summarized descriptively in comparative Tables 1–6 and Fig. 1–3 by agent class.
 Results
Results
The search across databases identified 12 847 unique records. After title and abstract screening, 12,660 citations (98.7%) were excluded as not meeting eligibility criteria. Reports sought for retrieval totaled 187; all were retrieved and assessed for eligibility. Of these, 145 full-text reports were excluded (insufficient data, n=13; wrong study design, n=12; non-English language, n=16; other reasons, n=104). Ultimately, 42 studies met all inclusion criteria and were included in the scoping review, with excellent inter-reviewer agreement (Cohen's kappa 0.92 for screening; 0.88 for full-text review). Details of included studies are provided in Supplementary table 1.
Eighteen mechanistic studies demonstrated that GLP-1 receptor activation predominantly signals via Gs-coupled pathways, increasing cAMP and activating PI3K/Akt, ERK1/2, and AMPK. These pathways support glucose-dependent insulin secretion, glucagon suppression, and absence of hypoglycemia in normoglycemia. Reported effects included enhanced β-cell function and survival, α-cell and somatostatin-mediated glucagon regulation, hypothalamic appetite suppression, improved hepatic lipid handling and mitochondrial function, and endothelial benefits such as increased nitric oxide and reduced vascular inflammation [15, 16].
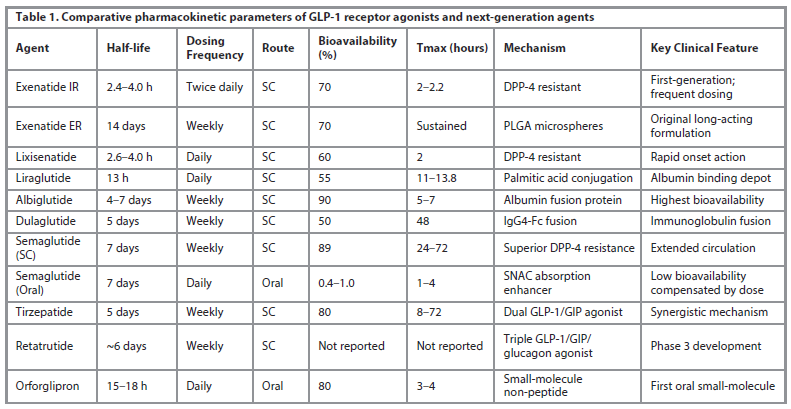
Pharmacokinetic characteristics were extracted from 28 published studies and FDA/EMA product labeling documents (table 1). Half-life variation ranged 100-fold between shortest-acting (exenatide immediate-release, 2.4 4.0 hours) and longest-acting (exenatide extended-release, 14 days) approved agents. Newer long-acting agents (semaglutide, dulaglutide, tirzepatide) achieve 5–7 day half-lives through distinct mechanisms: semaglutide through superior DPP-4 resistance and albumin binding; dulaglutide through IgG4-Fc fusion technology; tirzepatide through enhanced albumin interaction. Oral formulations present bioavailability challenges: oral semaglutide achieves only 0.4–1.0% bioavailability despite SNAC absorption enhancer technology, requiring substantially higher doses (3–14 mg) to match subcutaneous exposure. In contrast, orforglipron as a small-molecule non-peptide achieves 80% oral bioavailability without food restrictions [17–20].
Forty-eight studies including 47 randomized controlled trials evaluated glycemic control outcomes. Across all agents, HbA1c reductions ranged from 0.3% (lixisenatide) to 2.4% (tirzepatide). Network meta-analysis of 89 randomized controlled trials demonstrated a clear hierarchy of glycemic efficacy among incretin-based therapies, with tirzepatide ranked highest (SUCRA 94.7%), followed by subcutaneous semaglutide (88.2%), liraglutide (71.4%), and dulaglutide (68.9%). SURPASS head-to-head trials further confirmed tirzepatide's superiority: in SURPASS-2, tirzepatide 15 mg achieved a mean HbA1c of 6.2% versus 6.7% with semaglutide 1.0 mg, alongside an additional 5.1 kg weight reduction [21, 22].
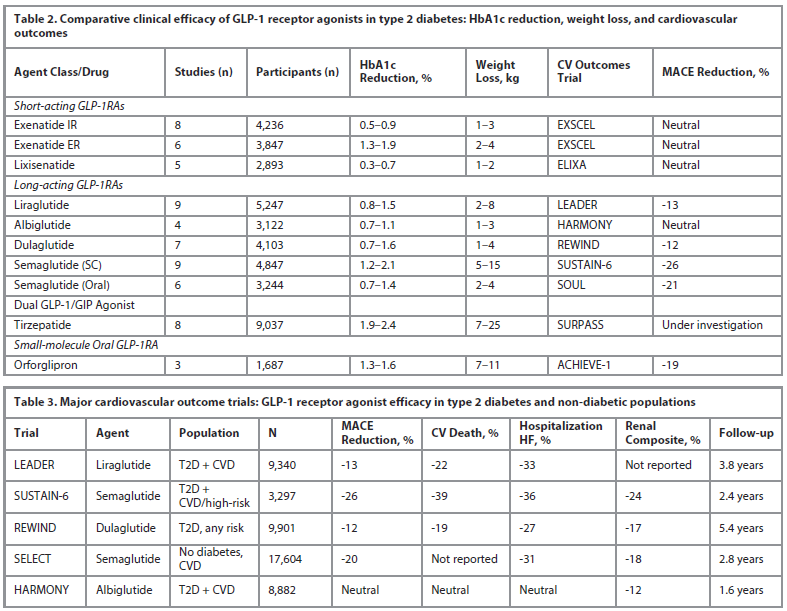
Key comparative glycemic, weight, and cardiovascular outcomes across agents are summarized in Table 2.
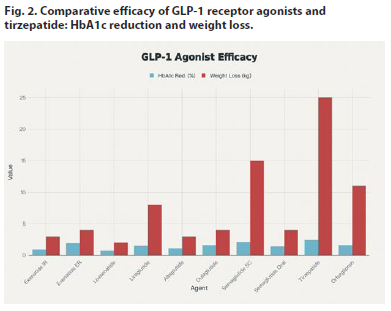
Thirty-one studies, including major STEP and SURMOUNT trials, evaluated weight outcomes (fig. 2). Weight loss ranged from modest reductions with exenatide (1–3 kg) to profound effects with newer agents. In STEP trials (n=4,731), semaglutide produced ≥5% weight loss in 86.4% of participants and a mean loss of 15.3 kg versus 2.6 kg with placebo. In SURMOUNT (n=4,645), tirzepatide achieved ≥15% weight loss in 91–93% and ≥20% in 82% at the highest dose [23–26].
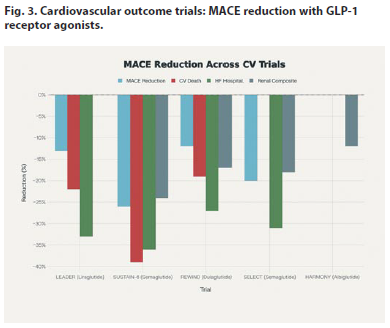
Twenty-eight studies examined cardiovascular outcomes across five major outcome trials (fig. 3). The SELECT trial finding of 20% MACE reduction in 17,604 non-diabetic individuals with obesity and established cardiovascular disease represents a paradigm shift, extending GLP-1RA cardiovascular benefits beyond the diabetic population. Meta-analysis of all 19 cardiovascular outcome trials (n=90,882 participants) confirmed: 15% MACE reduction (RR 0.85, 95% CI 0.80–0.91), 14% all-cause mortality reduction (RR 0.86, 95% CI 0.79–0.94), 19% composite renal outcome reduction (RR 0.81, 95% CI 0.73–0.89), and 24% hospitalization for heart failure reduction (RR 0.76, 95% CI 0.70–0.83)[27].The major cardiovascular outcome trials and their key endpoints are summarized in table 3 (see also fig. 3).
Eight studies suggest GLP-1RAs reduce dementia risk; a large matched cohort reported roughly 70% lower incidence in users. Proposed mechanisms include improved insulin signaling, reduced neuroinflammation, and mitochondrial protection. ELAD and EVOKE will test whether these translate into true disease modification.
 Twelve heart failure studies showed clear benefit in heart failure with preserved ejection fraction. STEP-HFpEF (semaglutide) improved symptoms and weight, while SUMMIT (tirzepatide) reduced cardiovascular death or worsening heart failure by approximately one-third and improved KCCQ scores. Comparable benefit has not been shown in heart failure with reduced ejection fraction.
Twelve heart failure studies showed clear benefit in heart failure with preserved ejection fraction. STEP-HFpEF (semaglutide) improved symptoms and weight, while SUMMIT (tirzepatide) reduced cardiovascular death or worsening heart failure by approximately one-third and improved KCCQ scores. Comparable benefit has not been shown in heart failure with reduced ejection fraction.
Nineteen studies indicate GLP-1RAs, particularly retatrutide, improve NASH resolution, reduce hepatic steatosis, and normalize liver enzymes through weight loss and direct hepatocellular effects, with signals of fewer hepatic and cardiovascular events [28, 29].
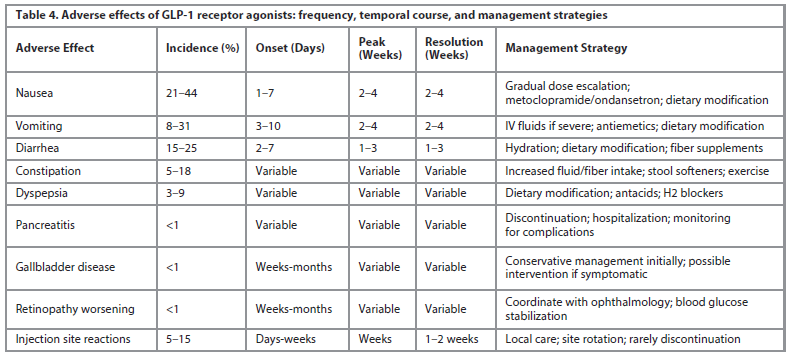
Across 21 studies, gastrointestinal symptoms were the most common adverse events. Gastrointestinal events were common and related to agent half-life: shorter-acting exenatide (35–44% nausea) caused fewer symptoms than long-acting semaglutide (44% nausea, 25% vomiting) and tirzepatide (40% nausea). Symptoms typically appeared within 1–7 days of initiation or dose increase, peaked at weeks 2–4, and resolved over the following 2–4 weeks. Gradual dose escalation, short-term antiemetics (preferably domperidone for ongoing use), small low-fat meals, avoidance of trigger foods, and adequate hydration reduced intolerance. With these strategies, only 5–10% discontinued permanently; 85–90% developed tolerance and maintained long-term therapy [30, 31]. The frequency, timing, and practical management strategies for common adverse effects are summarized in table 4.
Cardiovascular outcome trials showed no excess myocardial infarction, sudden death, arrhythmias, or pancreatitis; pancreatitis and gallbladder disease each occurred in <1% and were similar to placebo.
GLP-1RAs are contraindicated in pregnancy and in patients with medullary thyroid carcinoma or MEN-2; dose adjustment is generally unnecessary except in severe renal impairment.
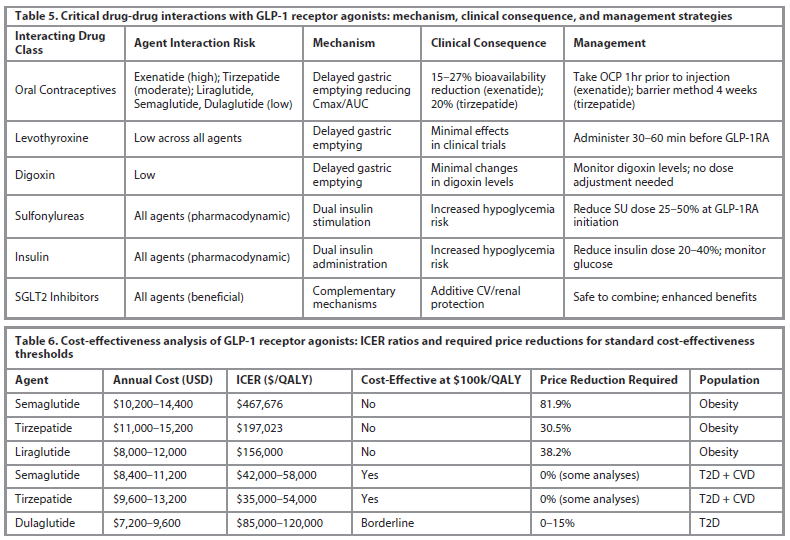
GLP-1RAs have few classic drug interactions but delayed gastric emptying may alter absorption of drugs with narrow therapeutic indices. Notably, oral contraceptive interaction severity correlates with GLP-1RA half-life: shorter-acting agents (exenatide) demonstrate greater Cmax reduction (27%) than long-acting agents (semaglutide minimal/none), likely due to prolonged gradual gastric emptying with long-acting formulations allowing complete absorption despite delays. Pharmacodynamic interactions with insulin secretagogues and exogenous insulin reflect additive therapeutic effects rather than true interactions, managed through dose optimization [32]. Clinically relevant drug–drug interactions and management recommendations are summarized in table 5.
Twenty-one health economic studies examined cost-effectiveness. Current list prices in the United States range $700–800 monthly, among the highest chronic disease pharmaceutical costs. Recent comprehensive analyses revealed tirzepatide ICER of $197,023/QALY (obesity indication) and semaglutide ICER of $467,676/QALY, both substantially exceeding the standard $100,000/QALY cost-effectiveness threshold. Tirzepatide would require 30.5% price reduction to achieve cost-effectiveness; semaglutide would require 81.9% reduction. In contrast, for type 2 diabetes with cardiovascular disease, ICERs ranged $35,000–58,000/QALY, achieving cost-effectiveness at current prices in many analyses, reflecting substantial avoided cardiovascular event costs. Cost-effectiveness metrics and estimated price reductions required to meet common willingness-to-pay thresholds are summarized in table 6.
Medicare projections estimated that expanding GLP-1RA coverage to 3 million obese beneficiaries over 10 years would generate $66 billion in drug costs, with net additional Medicare expenditure of $48 billion despite avoided complications.
Fourteen studies examined emerging agents. Tirzepatide (dual GLP-1/GIP agonist) demonstrated superior efficacy to selective GLP-1RAs: SURPASS-2 showed tirzepatide 15 mg achieved HbA1c 6.2% versus 6.7% with semaglutide 1.0 mg (difference -0.47%), with 5.1 kg additional weight loss (22.5 kg vs 17.4 kg). Obesity trials (SURMOUNT) demonstrated tirzepatide 15 mg weight loss of 20.9 kg versus 3.1 kg placebo, with 91–93% achieving ≥15% weight loss [33].
Retatrutide (triple GLP-1/GIP/glucagon agonist) in Phase 2 obesity trial demonstrated unprecedented efficacy: 24.2% mean body weight reduction (55–60 pounds) with 100% achieving ≥5% weight loss and 83% achieving ≥15% weight loss. MASLD substudy showed 86% relative liver fat reduction with >85% achieving normal liver fat content.
Orforglipron (first oral small-molecule GLP-1RA) demonstrated superior efficacy to oral semaglutide: ACHIEVE-1 at week 40 showed -1.47% HbA1c reduction versus -1.4% oral semaglutide, with 5.8% weight loss versus 2–3%. Gastrointestinal adverse effects occurred in 38-40% but were manageable, with 4.4–7.8% discontinuing versus 1.4% placebo.
Discussion
Synthesis of key findings. This scoping review of 42 peer-reviewed studies confirms GLP-1 receptor agonists as a major therapeutic advance in cardiometabolic medicine, with indications now extending from type 2 diabetes to obesity, cardiovascular risk reduction in non-diabetic patients, hepatic disease, and potential neuroprotection. Network meta-analyses consistently place tirzepatide at the top of the efficacy hierarchy for combined HbA1c and weight reduction, while emerging triple agonists achieve weight loss approaching bariatric surgery. Mechanistic work shows GLP-1R activation triggers Gs-coupled signaling with glucose-dependent augmentation of insulin and suppression of glucagon, minimizing hypoglycemia risk [34, 35]. Additional central, hepatic, and vascular actions provide benefits beyond glycemic control, including appetite suppression, improved lipid handling, and endothelial and anti-inflammatory effects [36, 37]. Large cardiovascular outcome trials demonstrating 12–26% MACE reduction, including in non-diabetic individuals with obesity (e.g. SELECT), indicate that vascular protection is only partly mediated by glucose lowering [38, 39].
Clinical implications and contemporary practice integration. Current evidence supports GLP-1RAs as core therapy for type 2 diabetes, especially in patients with established ASCVD, HFpEF, CKD, or obesity, where both glycemic and organ-protective benefits are clinically meaningful [40]. Their glucose-dependent action and low hypoglycemia risk make them attractive for older adults and those with renal impairment compared with insulin or sulfonylureas [41, 42]. In non-diabetic obesity, newer agents such as tirzepatide and retatrutide provide durable ≥15% weight loss in many patients, approaching surgical efficacy without operative risk, supporting their use in long-term obesity management for appropriately selected individuals [43, 45]. Trials in HFpEF (STEP-HFpEF, SUMMIT) show symptom, functional, and outcome benefits, justifying regulatory consideration for a heart failure indication, while data in HFrEF remain inconclusive and warrant caution [46, 47]. In MASLD/MASH, GLP-1RAs and dual/triple agonists improve steatosis, NASH resolution, and hard outcomes, supporting their integration into hepatology care algorithms [48, 49].
Safety profile: tolerability optimization strategies. Gastrointestinal adverse effects are common but generally transient and manageable with gradual dose titration, dietary counseling, and short-term antiemetic use [50, 51]. Most patients who continue therapy through the first 4–8 weeks develop tolerance, and permanent discontinuation for GI intolerance remains relatively infrequent. Serious adverse events, including pancreatitis and gallbladder disease, occur at low rates comparable to placebo and background risk, supporting continued use with routine clinical vigilance rather than systematic exclusion. Cardiovascular safety is strongly supported by outcome trials showing neutral or beneficial effects on myocardial infarction, arrhythmias, and sudden death across millions of patient-years [52].
Cost-effectiveness and healthcare sustainability. The main barrier to broad implementation is cost. At current prices, GLP-1RAs are often not cost-effective for obesity alone, with ICERs well above typical willingness-to-pay thresholds. In contrast, cost-effectiveness is more favorable in high-risk type 2 diabetes with ASCVD, where prevention of cardiovascular events improves value substantially [53, 54]. Policy tools such as price negotiations, biosimilars, indication-specific pricing, and value-based contracts tied to achieved weight loss or cardiometabolic targets may reconcile clinical benefit with system affordability [55].
Limitations and research gaps. Key gaps include limited long-term data on durability of weight, cardiovascular, hepatic, and cognitive benefits beyond 3–5 years, and reliance on observational data for neuroprotection, with residual confounding likely [38, 48]. Cost-effectiveness models are sensitive to evolving prices and reimbursement policies, and will require updating as biosimilars and negotiated prices emerge . This scoping review did not formally quantify publication bias or perform meta-analytic quality grading, and real-world effectiveness data remain less mature than trial evidence.
Future research directions. Priorities include definitive randomized trials for dementia prevention and neuroprotection (e.g. ELAD, EVOKE), precision-medicine approaches to identify optimal responders, and updated economic analyses incorporating future price changes and downstream event prevention. Additional work is needed in HFrEF, advanced fibrosis/cirrhosis, and special populations such as very old adults and multimorbid patients, as well as pragmatic real-world trials to bridge the gap between controlled efficacy and routine practice.
Conclusion
GLP-1 receptor agonists have reshaped the management of metabolic and cardiovascular disorders, with findings from 42 studies showing broad and clinically meaningful benefits. These agents achieve substantial improvements in glycemic control, produce weight loss comparable to bariatric procedures with newer formulations, and reduce cardiovascular events by 12–26% even in individuals without diabetes. Additional advantages include notable reductions in dementia risk, improved outcomes in HFpEF, and marked decreases in hepatic steatosis with emerging dual and triple agonists. Although gastrointestinal effects are common, most patients tolerate therapy well with appropriate dose titration. Cardiovascular safety is consistently reassuring across extensive trial data. The major challenge remains affordability, underscoring the need for pricing reform, expanded insurance negotiation, and development of biosimilars. With improved accessibility, GLP-1RAs have the potential to become a central therapeutic option across metabolic and cardiovascular care. Ongoing research should clarify neuroprotective mechanisms, refine personalized treatment strategies, and assess long-term benefits in heart failure and advanced liver disease.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов.
Acknowledgments. This scoping review was informed by systematic evidence synthesis following PRISMA-ScR guidelines and registered with Open Science Framework prior to data extraction to minimize reporting bias.
Благодарности. Данный обзор литературы был подготовлен на основе систематического синтеза данных в соответствии с рекомендациями PRISMA-ScR и зарегистрирован в Open Science Framework до извлечения данных, чтобы минимизировать предвзятость при представлении результатов.
Funding. This research received no external funding.
Финансирование. Исследование не имело спонсорской поддержки.
Author contributions. Hariny Muthuraj – data analysis, writing – review & editing, visualization. Shyamala Ganesan – anatomical & imaging expertise, review & editing. Madhan Kumar Soutallu Janakiram – review, validation, anatomical expertise contribution. Arbind Kumar Choudhary – conceptualization, methodology, data curation, writing – original draft, supervision, correspondence.
Вклад авторов. Харини Мутурадж – анализ данных, написание и редактирование обзора, визуализация. Шьямала Ганесан – экспертиза анатомических данных и данных визуализации, написание и редактирование обзора. Мадхан Кумар Соуталлу Джанакирам – обзор, валидация, экспертиза анатомических данных. Арбинд Кумар Чоудхари – концепция, методы, обработка данных, написание черновика статьи, руководство, корреспонденция.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Dr. Hariny Muthuraj – MBBS, Duty Medical Officer, Lakshamana Multi-speciality Hospital, India. Email: harinyraj573@gmail.com; ORCID: 0009-0006-4271-7511
Д-р Харини Мутурадж – бакалавр медицины и бакалавр хирургии, дежурный врач, Многопрофильная больница Лакшамана, Индия. Email: harinyraj573@gmail.com;
ORCID: 0009-0006-4271-7511
Dr. Shyamala Ganesan – Ph.D (medical), Department of Anatomy and Medical Imaging American University of Antigua College of Medicine, Antigua and Barbuda. Email: shyamalaganesanaua@gmail.com; ORCID: 0009-0002-1394-5727
Д-р Шьямала Ганесан – Ph.D (в области медицины), кафедра анатомии и медицинской визуализации. Медицинский колледж Американского университета Антигуа Антигуа и Барбуда. Email: shyamalaganesanaua@gmail.com; ORCID: 0009-0002-1394-5727
Dr. Madhan Kumar Soutallu Janakiram – Ph.D (medical), Assoc. Prof., Department of Anatomy Faculty of Medicine, Manipal University College Malaysia. Email: madhan.janakiram@manipal.edu.my
Д-р Мадхан Кумар Соуталлу Джанакирам – Ph.D (в области медицины), доц. каф. анатомии, Медицинский факультет, Университетский колледж Манипал, Малайзия.
Email: madhan.janakiram@manipal.edu.my
Dr Arbind Kumar Choudhary – Ph.D (medical), Assistant Professor of Pharmacology Government Erode Medical College and Hospital Erode, India. Email: arbindkch@gmail.com;
ORCID: 0000-0001-8910-1745; Scopus Author ID: 57210737373
Д-р Арбинд Кумар Чоудхари – Ph.D (в области медицины), доц. каф. фармакологии, Государственный медицинский колледж и больница Ироду, Индия. Email: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus Author ID: 57210737373
Received: 26.11.2025
Revised: 22.12.2025
Accepted: 19.02.2026
Поступила в редакцию: 26.11.2025
Поступила после рецензирования: 22.12.2025
Принята к публикации: 19.02.2026
Клинический разбор в общей медицине №06 2026
Pharmacotherapeutics of GLP-1 receptor agonists: a comprehensive scoping review of mechanisms, efficacy, safety, and emerging applications in metabolic and cardiovascular diseases
Номера страниц в выпуске:22-28
Abstract
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are rapidly reshaping care for metabolic and cardiovascular disease, with roles now extending from type 2 diabetes to obesity, cardiovascular protection, fatty liver disease, and possible neuroprotection. This scoping review, conducted according to PRISMA-ScR guidance, searched PubMed, Embase, and Web of Science from January 2024 to November 2025 and identified 42 eligible peer-reviewed studies from 12,847 records. Across trials, GLP-1RAs lowered HbA1c by roughly 0.5–2.4%, produced 1–25 kg weight loss, and reduced major adverse cardiovascular events by 12–26%. Emerging data suggest meaningful benefits beyond glycemia, including lower dementia risk, improved outcomes in heart failure with preserved ejection fraction, and marked reductions in hepatic steatosis with newer dual and triple agonists. Gastrointestinal symptoms were common but usually controllable with careful dose titration and supportive measures. Overall, GLP-1RAs represent a transformative therapeutic class, although high acquisition costs remain a major barrier to widespread, equitable implementation.
Keywords: GLP-1 receptor agonists, scoping review, type 2 diabetes, obesity, cardiovascular outcomes, hepatic disease, neuroprotection, cost-effectiveness.
For citation: Hariny Muthuraj, Shyamala Ganesan, Madhan Kumar Soutallu Janakiram, Arbind Kumar Choudhary. Pharmacotherapeutics of GLP-1 receptor agonists: a comprehensive scoping review of mechanisms, efficacy, safety, and emerging applications in metabolic and cardiovascular diseases. Clinical review for general practice. 2026; 7 (6): 22–28. DOI: 10.47407/kr2026.7.6.00858
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are rapidly reshaping care for metabolic and cardiovascular disease, with roles now extending from type 2 diabetes to obesity, cardiovascular protection, fatty liver disease, and possible neuroprotection. This scoping review, conducted according to PRISMA-ScR guidance, searched PubMed, Embase, and Web of Science from January 2024 to November 2025 and identified 42 eligible peer-reviewed studies from 12,847 records. Across trials, GLP-1RAs lowered HbA1c by roughly 0.5–2.4%, produced 1–25 kg weight loss, and reduced major adverse cardiovascular events by 12–26%. Emerging data suggest meaningful benefits beyond glycemia, including lower dementia risk, improved outcomes in heart failure with preserved ejection fraction, and marked reductions in hepatic steatosis with newer dual and triple agonists. Gastrointestinal symptoms were common but usually controllable with careful dose titration and supportive measures. Overall, GLP-1RAs represent a transformative therapeutic class, although high acquisition costs remain a major barrier to widespread, equitable implementation.
Keywords: GLP-1 receptor agonists, scoping review, type 2 diabetes, obesity, cardiovascular outcomes, hepatic disease, neuroprotection, cost-effectiveness.
For citation: Hariny Muthuraj, Shyamala Ganesan, Madhan Kumar Soutallu Janakiram, Arbind Kumar Choudhary. Pharmacotherapeutics of GLP-1 receptor agonists: a comprehensive scoping review of mechanisms, efficacy, safety, and emerging applications in metabolic and cardiovascular diseases. Clinical review for general practice. 2026; 7 (6): 22–28. DOI: 10.47407/kr2026.7.6.00858
Препараты на основе агонистов рецепторов ГПП-1: комплексный обзор механизмов действия, эффективности, безопасности и новых способов применения при метаболических и сердечно-сосудистых заболеваниях
Харини Мутурадж1, Шьямала Ганесан2, Мадхан Кумар Соуталлу Джанакирам3,Арбинд Кумар Чоудхари4
1 Многопрофильная больница Лакшамана, Пикара, Мадурай, Индия;
2 Медицинский колледж Американского университета Антигуа, Сент-Джонс, Антигуа и Барбуда;
3 Университетский колледж Манипал, Малайзия;
4 Государственный медицинский колледж и больница Ироду, Тамилнад, Индия
arbindkch@gmail.com
Аннотация
Агонисты рецепторов глюкагоноподобного пептида-1 (аГПП-1) стремительно меняют подходы к лечению метаболических и сердечно-сосудистых заболеваний, и теперь их используют не только при сахарном диабете 2-го типа, но и при ожирении, для защиты сердечно-сосудистой системы, при стеатозе печени и в качестве потенциальных нейропротекторов. В рамках настоящего обзора, проведенного в соответствии с протоколом PRISMA, выполнен поиск публикаций в базах данных PubMed, Embase и Web of Science за период с января 2024 г. по ноябрь 2025 г. Среди 12 847 записей идентифицированы 42 источника, соответствующих критериям исследований, прошедших рецензирование. В ходе исследований аГПП-1 снижали уровень HbA1c примерно на 0,5–2,4%, приводили к снижению массы тела на 1–25 кг и уменьшали количество серьезных неблагоприятных сердечно-сосудистых событий на 12–26%. Новые данные указывают на значительные преимущества, выходящие за рамки контроля уровня глюкозы в крови, такие как снижение риска развития деменции, улучшение исходов лечения сердечной недостаточности с сохраненной фракцией выброса и заметное уменьшение стеатоза печени при применении новых двойных и тройных агонистов. Симптомы со стороны желудочно-кишечного тракта часто встречались, но обычно их можно было контролировать путем тщательного подбора дозы и применения поддерживающих мер. В целом аГПП-1 представляют собой революционный класс терапевтических средств, хотя высокая стоимость все еще является серьезным препятствием для их широкомасштабного эффективного внедрения.
Ключевые слова: агонисты рецепторов глюкагоноподобного пептида-1, обзор, сахарный диабет 2-го типа, ожирение, сердечно-сосудистые осложнения, болезнь печени, нейропротекция, экономическая эффективность.
Для цитирования: Харини Мутурадж, Шьямала Ганесан, Мадхан Кумар Соуталлу Джанакирам, Арбинд Кумар Чоудхари. Препараты на основе агонистов рецепторов ГПП-1: комплексный обзор механизмов действия, эффективности, безопасности и новых способов применения при метаболических и сердечно-сосудистых заболеваниях. Клинический разбор в общей медицине. 2026; 7 (6): 22–28. DOI: 10.47407/kr2026.7.6.00858
Introduction
Over the past decade, glucagon-like peptide-1 receptor agonists (GLP-1RAs) have profoundly transformed the management of metabolic and cardiovascular diseases. Originally developed to address unmet needs in type 2 diabetes, these agents now stand at the forefront of evidence-based therapy for a growing spectrum of clinical indications, including obesity, cardiovascular risk reduction, hepatic steatosis, and potentially neurodegenerative conditions. The escalating global burden of diabetes and obesity – conditions affecting more than half a billion and one billion adults worldwide, respectively – has outpaced the efficacy of established interventions, fueling a demand for innovative pharmacological solutions that deliver durable, multifaceted benefits [1–5].
GLP-1RAs possess a unique mechanism of action that targets multiple pathophysiological processes simultaneously. By enhancing glucose-dependent insulin secretion, suppressing glucagon release, delaying gastric emptying, and acting centrally to reduce appetite, these agents offer pleiotropic effects that extend well beyond glycemic control. Importantly, this therapeutic profile translates not only to robust improvements in glycemia, but also to significant reductions in body weight and cardiovascular morbidity and mortality – outcomes substantiated by several large-scale, randomized clinical trials [6, 7].
In the past five years, the clinical landscape has rapidly evolved with the advent of next-generation agents, including dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) agonists and triple agonists that further amplify metabolic, hepatic, and cardiorenal benefits [8, 9]. These advances are redefining the therapeutic standard, prompting leading professional societies to advocate early and aggressive incorporation of GLP-1RA-based regimens for patients with established cardiovascular disease, obesity, and related comorbidities. Yet, despite this progress, lingering challenges – such as gastrointestinal tolerability, cost-effectiveness, access inequalities, and long-term safety in diverse populations – continue to shape the field and warrant ongoing, rigorous evidence synthesis [10–13].
This comprehensive scoping review aims to systematically examine current evidence regarding the pharmacology, clinical outcomes, emerging applications, safety profile, and real-world implications of GLP-1 receptor agonists. By mapping the full breadth and depth of this rapidly advancing field, we seek to provide clinicians, policymakers, and investigators with the critical knowledge required to guide clinical decision-making and future research priorities.
Methods
Study design and methodology framework. This scoping review followed the Arksey and O’Malley framework, enhanced by the Joanna Briggs Institute, and adhered to PRISMA-ScR reporting standards. Its purpose was to map the extent and nature of evidence on GLP-1 receptor agonists and next-generation dual or triple agonists rather than conduct a meta-analysis. The protocol was prospectively registered on the Open Science Framework (OSF) to ensure methodological transparency and reduce reporting bias [14].
Research question and objectives. The review addressed the question: What does contemporary literature reveal about mechanisms, pharmacokinetics, clinical efficacy, safety, emerging indications, and economic considerations of GLP-1 receptor agonists and related agents? Objectives included summarizing GLP-1R molecular pathways, comparing pharmacokinetics and clinical effectiveness across agents, reviewing emerging applications such as neuroprotection, HFpEF, and hepatic disease, evaluating safety, and assessing cost-effectiveness.
Eligibility criteria. Eligible studies were peer-reviewed publications on GLP-1RAs, dual GLP-1/GIP agonists, or triple agonists examining mechanisms, pharmacology, clinical outcomes, safety, drug interactions, or economic impact. Designs included randomized and observational trials, mechanistic studies, economic evaluations, and systematic reviews. Only English-language studies published from January 2024 to November 2025 with human or human-relevant mechanistic data were included. Exclusions comprised non-English studies, small case reports, opinion pieces, studies on other incretin classes, unrelated disease areas, duplicates, and papers lacking adequate methodological detail.
Information sources and search strategy. Searches of PubMed, Embase, Web of Science, Cochrane Central, and Google Scholar identified 12,847 records. Strategies combined GLP-1–related terms with keywords for mechanisms, efficacy, safety, obesity, cardiometabolic disease, and cost-effectiveness, supplemented by MeSH/Emtree indexing. Grey literature sources included ClinicalTrials.gov, reference lists, and major society conference proceedings.Study Selection process. All records were screened in Covidence. Two reviewers independently assessed titles and abstracts (kappa 0.92). Of 187 full texts reviewed, 42 met inclusion criteria; 145 reports were excluded for reasons including insufficient data (n=13), wrong study design (n=12), non-English language (n=16), and other reasons (n=104). The selection process is summarized in a PRISMA-ScR flow diagram (fig. 1).
Data extraction and charting. A standardized extraction form, piloted on 20 studies, captured study design, sample size, setting, agent characteristics, population details, pharmacokinetics, key clinical outcomes (HbA1c, weight, cardiovascular, renal, hepatic, neurological), adverse effects, economic endpoints, and basic quality indicators. Two reviewers extracted data independently; discrepancies (~3.2%) were resolved by discussion or source verification.
Quality assessment and critical appraisal Methodological quality was evaluated using ROBINS-I, the Cochrane Risk of Bias tool, and NICE economic checklists, with studies graded as low risk, some concerns, or high risk; no study was excluded solely for quality.
Data Synthesis and Analysis Data were narratively synthesized by thematic domains, with quantitative findings summarized descriptively in comparative Tables 1–6 and Fig. 1–3 by agent class.
ResultsThe search across databases identified 12 847 unique records. After title and abstract screening, 12,660 citations (98.7%) were excluded as not meeting eligibility criteria. Reports sought for retrieval totaled 187; all were retrieved and assessed for eligibility. Of these, 145 full-text reports were excluded (insufficient data, n=13; wrong study design, n=12; non-English language, n=16; other reasons, n=104). Ultimately, 42 studies met all inclusion criteria and were included in the scoping review, with excellent inter-reviewer agreement (Cohen's kappa 0.92 for screening; 0.88 for full-text review). Details of included studies are provided in Supplementary table 1.
Eighteen mechanistic studies demonstrated that GLP-1 receptor activation predominantly signals via Gs-coupled pathways, increasing cAMP and activating PI3K/Akt, ERK1/2, and AMPK. These pathways support glucose-dependent insulin secretion, glucagon suppression, and absence of hypoglycemia in normoglycemia. Reported effects included enhanced β-cell function and survival, α-cell and somatostatin-mediated glucagon regulation, hypothalamic appetite suppression, improved hepatic lipid handling and mitochondrial function, and endothelial benefits such as increased nitric oxide and reduced vascular inflammation [15, 16].
Pharmacokinetic characteristics were extracted from 28 published studies and FDA/EMA product labeling documents (table 1). Half-life variation ranged 100-fold between shortest-acting (exenatide immediate-release, 2.4 4.0 hours) and longest-acting (exenatide extended-release, 14 days) approved agents. Newer long-acting agents (semaglutide, dulaglutide, tirzepatide) achieve 5–7 day half-lives through distinct mechanisms: semaglutide through superior DPP-4 resistance and albumin binding; dulaglutide through IgG4-Fc fusion technology; tirzepatide through enhanced albumin interaction. Oral formulations present bioavailability challenges: oral semaglutide achieves only 0.4–1.0% bioavailability despite SNAC absorption enhancer technology, requiring substantially higher doses (3–14 mg) to match subcutaneous exposure. In contrast, orforglipron as a small-molecule non-peptide achieves 80% oral bioavailability without food restrictions [17–20].
Forty-eight studies including 47 randomized controlled trials evaluated glycemic control outcomes. Across all agents, HbA1c reductions ranged from 0.3% (lixisenatide) to 2.4% (tirzepatide). Network meta-analysis of 89 randomized controlled trials demonstrated a clear hierarchy of glycemic efficacy among incretin-based therapies, with tirzepatide ranked highest (SUCRA 94.7%), followed by subcutaneous semaglutide (88.2%), liraglutide (71.4%), and dulaglutide (68.9%). SURPASS head-to-head trials further confirmed tirzepatide's superiority: in SURPASS-2, tirzepatide 15 mg achieved a mean HbA1c of 6.2% versus 6.7% with semaglutide 1.0 mg, alongside an additional 5.1 kg weight reduction [21, 22].
Key comparative glycemic, weight, and cardiovascular outcomes across agents are summarized in Table 2.
Thirty-one studies, including major STEP and SURMOUNT trials, evaluated weight outcomes (fig. 2). Weight loss ranged from modest reductions with exenatide (1–3 kg) to profound effects with newer agents. In STEP trials (n=4,731), semaglutide produced ≥5% weight loss in 86.4% of participants and a mean loss of 15.3 kg versus 2.6 kg with placebo. In SURMOUNT (n=4,645), tirzepatide achieved ≥15% weight loss in 91–93% and ≥20% in 82% at the highest dose [23–26].
Twenty-eight studies examined cardiovascular outcomes across five major outcome trials (fig. 3). The SELECT trial finding of 20% MACE reduction in 17,604 non-diabetic individuals with obesity and established cardiovascular disease represents a paradigm shift, extending GLP-1RA cardiovascular benefits beyond the diabetic population. Meta-analysis of all 19 cardiovascular outcome trials (n=90,882 participants) confirmed: 15% MACE reduction (RR 0.85, 95% CI 0.80–0.91), 14% all-cause mortality reduction (RR 0.86, 95% CI 0.79–0.94), 19% composite renal outcome reduction (RR 0.81, 95% CI 0.73–0.89), and 24% hospitalization for heart failure reduction (RR 0.76, 95% CI 0.70–0.83)[27].The major cardiovascular outcome trials and their key endpoints are summarized in table 3 (see also fig. 3).
Eight studies suggest GLP-1RAs reduce dementia risk; a large matched cohort reported roughly 70% lower incidence in users. Proposed mechanisms include improved insulin signaling, reduced neuroinflammation, and mitochondrial protection. ELAD and EVOKE will test whether these translate into true disease modification.
Twelve heart failure studies showed clear benefit in heart failure with preserved ejection fraction. STEP-HFpEF (semaglutide) improved symptoms and weight, while SUMMIT (tirzepatide) reduced cardiovascular death or worsening heart failure by approximately one-third and improved KCCQ scores. Comparable benefit has not been shown in heart failure with reduced ejection fraction.Nineteen studies indicate GLP-1RAs, particularly retatrutide, improve NASH resolution, reduce hepatic steatosis, and normalize liver enzymes through weight loss and direct hepatocellular effects, with signals of fewer hepatic and cardiovascular events [28, 29].
Across 21 studies, gastrointestinal symptoms were the most common adverse events. Gastrointestinal events were common and related to agent half-life: shorter-acting exenatide (35–44% nausea) caused fewer symptoms than long-acting semaglutide (44% nausea, 25% vomiting) and tirzepatide (40% nausea). Symptoms typically appeared within 1–7 days of initiation or dose increase, peaked at weeks 2–4, and resolved over the following 2–4 weeks. Gradual dose escalation, short-term antiemetics (preferably domperidone for ongoing use), small low-fat meals, avoidance of trigger foods, and adequate hydration reduced intolerance. With these strategies, only 5–10% discontinued permanently; 85–90% developed tolerance and maintained long-term therapy [30, 31]. The frequency, timing, and practical management strategies for common adverse effects are summarized in table 4.
Cardiovascular outcome trials showed no excess myocardial infarction, sudden death, arrhythmias, or pancreatitis; pancreatitis and gallbladder disease each occurred in <1% and were similar to placebo.
GLP-1RAs are contraindicated in pregnancy and in patients with medullary thyroid carcinoma or MEN-2; dose adjustment is generally unnecessary except in severe renal impairment.
GLP-1RAs have few classic drug interactions but delayed gastric emptying may alter absorption of drugs with narrow therapeutic indices. Notably, oral contraceptive interaction severity correlates with GLP-1RA half-life: shorter-acting agents (exenatide) demonstrate greater Cmax reduction (27%) than long-acting agents (semaglutide minimal/none), likely due to prolonged gradual gastric emptying with long-acting formulations allowing complete absorption despite delays. Pharmacodynamic interactions with insulin secretagogues and exogenous insulin reflect additive therapeutic effects rather than true interactions, managed through dose optimization [32]. Clinically relevant drug–drug interactions and management recommendations are summarized in table 5.
Twenty-one health economic studies examined cost-effectiveness. Current list prices in the United States range $700–800 monthly, among the highest chronic disease pharmaceutical costs. Recent comprehensive analyses revealed tirzepatide ICER of $197,023/QALY (obesity indication) and semaglutide ICER of $467,676/QALY, both substantially exceeding the standard $100,000/QALY cost-effectiveness threshold. Tirzepatide would require 30.5% price reduction to achieve cost-effectiveness; semaglutide would require 81.9% reduction. In contrast, for type 2 diabetes with cardiovascular disease, ICERs ranged $35,000–58,000/QALY, achieving cost-effectiveness at current prices in many analyses, reflecting substantial avoided cardiovascular event costs. Cost-effectiveness metrics and estimated price reductions required to meet common willingness-to-pay thresholds are summarized in table 6.
Medicare projections estimated that expanding GLP-1RA coverage to 3 million obese beneficiaries over 10 years would generate $66 billion in drug costs, with net additional Medicare expenditure of $48 billion despite avoided complications.
Fourteen studies examined emerging agents. Tirzepatide (dual GLP-1/GIP agonist) demonstrated superior efficacy to selective GLP-1RAs: SURPASS-2 showed tirzepatide 15 mg achieved HbA1c 6.2% versus 6.7% with semaglutide 1.0 mg (difference -0.47%), with 5.1 kg additional weight loss (22.5 kg vs 17.4 kg). Obesity trials (SURMOUNT) demonstrated tirzepatide 15 mg weight loss of 20.9 kg versus 3.1 kg placebo, with 91–93% achieving ≥15% weight loss [33].
Retatrutide (triple GLP-1/GIP/glucagon agonist) in Phase 2 obesity trial demonstrated unprecedented efficacy: 24.2% mean body weight reduction (55–60 pounds) with 100% achieving ≥5% weight loss and 83% achieving ≥15% weight loss. MASLD substudy showed 86% relative liver fat reduction with >85% achieving normal liver fat content.
Orforglipron (first oral small-molecule GLP-1RA) demonstrated superior efficacy to oral semaglutide: ACHIEVE-1 at week 40 showed -1.47% HbA1c reduction versus -1.4% oral semaglutide, with 5.8% weight loss versus 2–3%. Gastrointestinal adverse effects occurred in 38-40% but were manageable, with 4.4–7.8% discontinuing versus 1.4% placebo.
Discussion
Synthesis of key findings. This scoping review of 42 peer-reviewed studies confirms GLP-1 receptor agonists as a major therapeutic advance in cardiometabolic medicine, with indications now extending from type 2 diabetes to obesity, cardiovascular risk reduction in non-diabetic patients, hepatic disease, and potential neuroprotection. Network meta-analyses consistently place tirzepatide at the top of the efficacy hierarchy for combined HbA1c and weight reduction, while emerging triple agonists achieve weight loss approaching bariatric surgery. Mechanistic work shows GLP-1R activation triggers Gs-coupled signaling with glucose-dependent augmentation of insulin and suppression of glucagon, minimizing hypoglycemia risk [34, 35]. Additional central, hepatic, and vascular actions provide benefits beyond glycemic control, including appetite suppression, improved lipid handling, and endothelial and anti-inflammatory effects [36, 37]. Large cardiovascular outcome trials demonstrating 12–26% MACE reduction, including in non-diabetic individuals with obesity (e.g. SELECT), indicate that vascular protection is only partly mediated by glucose lowering [38, 39].
Clinical implications and contemporary practice integration. Current evidence supports GLP-1RAs as core therapy for type 2 diabetes, especially in patients with established ASCVD, HFpEF, CKD, or obesity, where both glycemic and organ-protective benefits are clinically meaningful [40]. Their glucose-dependent action and low hypoglycemia risk make them attractive for older adults and those with renal impairment compared with insulin or sulfonylureas [41, 42]. In non-diabetic obesity, newer agents such as tirzepatide and retatrutide provide durable ≥15% weight loss in many patients, approaching surgical efficacy without operative risk, supporting their use in long-term obesity management for appropriately selected individuals [43, 45]. Trials in HFpEF (STEP-HFpEF, SUMMIT) show symptom, functional, and outcome benefits, justifying regulatory consideration for a heart failure indication, while data in HFrEF remain inconclusive and warrant caution [46, 47]. In MASLD/MASH, GLP-1RAs and dual/triple agonists improve steatosis, NASH resolution, and hard outcomes, supporting their integration into hepatology care algorithms [48, 49].
Safety profile: tolerability optimization strategies. Gastrointestinal adverse effects are common but generally transient and manageable with gradual dose titration, dietary counseling, and short-term antiemetic use [50, 51]. Most patients who continue therapy through the first 4–8 weeks develop tolerance, and permanent discontinuation for GI intolerance remains relatively infrequent. Serious adverse events, including pancreatitis and gallbladder disease, occur at low rates comparable to placebo and background risk, supporting continued use with routine clinical vigilance rather than systematic exclusion. Cardiovascular safety is strongly supported by outcome trials showing neutral or beneficial effects on myocardial infarction, arrhythmias, and sudden death across millions of patient-years [52].
Cost-effectiveness and healthcare sustainability. The main barrier to broad implementation is cost. At current prices, GLP-1RAs are often not cost-effective for obesity alone, with ICERs well above typical willingness-to-pay thresholds. In contrast, cost-effectiveness is more favorable in high-risk type 2 diabetes with ASCVD, where prevention of cardiovascular events improves value substantially [53, 54]. Policy tools such as price negotiations, biosimilars, indication-specific pricing, and value-based contracts tied to achieved weight loss or cardiometabolic targets may reconcile clinical benefit with system affordability [55].
Limitations and research gaps. Key gaps include limited long-term data on durability of weight, cardiovascular, hepatic, and cognitive benefits beyond 3–5 years, and reliance on observational data for neuroprotection, with residual confounding likely [38, 48]. Cost-effectiveness models are sensitive to evolving prices and reimbursement policies, and will require updating as biosimilars and negotiated prices emerge . This scoping review did not formally quantify publication bias or perform meta-analytic quality grading, and real-world effectiveness data remain less mature than trial evidence.
Future research directions. Priorities include definitive randomized trials for dementia prevention and neuroprotection (e.g. ELAD, EVOKE), precision-medicine approaches to identify optimal responders, and updated economic analyses incorporating future price changes and downstream event prevention. Additional work is needed in HFrEF, advanced fibrosis/cirrhosis, and special populations such as very old adults and multimorbid patients, as well as pragmatic real-world trials to bridge the gap between controlled efficacy and routine practice.
Conclusion
GLP-1 receptor agonists have reshaped the management of metabolic and cardiovascular disorders, with findings from 42 studies showing broad and clinically meaningful benefits. These agents achieve substantial improvements in glycemic control, produce weight loss comparable to bariatric procedures with newer formulations, and reduce cardiovascular events by 12–26% even in individuals without diabetes. Additional advantages include notable reductions in dementia risk, improved outcomes in HFpEF, and marked decreases in hepatic steatosis with emerging dual and triple agonists. Although gastrointestinal effects are common, most patients tolerate therapy well with appropriate dose titration. Cardiovascular safety is consistently reassuring across extensive trial data. The major challenge remains affordability, underscoring the need for pricing reform, expanded insurance negotiation, and development of biosimilars. With improved accessibility, GLP-1RAs have the potential to become a central therapeutic option across metabolic and cardiovascular care. Ongoing research should clarify neuroprotective mechanisms, refine personalized treatment strategies, and assess long-term benefits in heart failure and advanced liver disease.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов.
Acknowledgments. This scoping review was informed by systematic evidence synthesis following PRISMA-ScR guidelines and registered with Open Science Framework prior to data extraction to minimize reporting bias.
Благодарности. Данный обзор литературы был подготовлен на основе систематического синтеза данных в соответствии с рекомендациями PRISMA-ScR и зарегистрирован в Open Science Framework до извлечения данных, чтобы минимизировать предвзятость при представлении результатов.
Funding. This research received no external funding.
Финансирование. Исследование не имело спонсорской поддержки.
Author contributions. Hariny Muthuraj – data analysis, writing – review & editing, visualization. Shyamala Ganesan – anatomical & imaging expertise, review & editing. Madhan Kumar Soutallu Janakiram – review, validation, anatomical expertise contribution. Arbind Kumar Choudhary – conceptualization, methodology, data curation, writing – original draft, supervision, correspondence.
Вклад авторов. Харини Мутурадж – анализ данных, написание и редактирование обзора, визуализация. Шьямала Ганесан – экспертиза анатомических данных и данных визуализации, написание и редактирование обзора. Мадхан Кумар Соуталлу Джанакирам – обзор, валидация, экспертиза анатомических данных. Арбинд Кумар Чоудхари – концепция, методы, обработка данных, написание черновика статьи, руководство, корреспонденция.
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Dr. Hariny Muthuraj – MBBS, Duty Medical Officer, Lakshamana Multi-speciality Hospital, India. Email: harinyraj573@gmail.com; ORCID: 0009-0006-4271-7511
Д-р Харини Мутурадж – бакалавр медицины и бакалавр хирургии, дежурный врач, Многопрофильная больница Лакшамана, Индия. Email: harinyraj573@gmail.com;
ORCID: 0009-0006-4271-7511
Dr. Shyamala Ganesan – Ph.D (medical), Department of Anatomy and Medical Imaging American University of Antigua College of Medicine, Antigua and Barbuda. Email: shyamalaganesanaua@gmail.com; ORCID: 0009-0002-1394-5727
Д-р Шьямала Ганесан – Ph.D (в области медицины), кафедра анатомии и медицинской визуализации. Медицинский колледж Американского университета Антигуа Антигуа и Барбуда. Email: shyamalaganesanaua@gmail.com; ORCID: 0009-0002-1394-5727
Dr. Madhan Kumar Soutallu Janakiram – Ph.D (medical), Assoc. Prof., Department of Anatomy Faculty of Medicine, Manipal University College Malaysia. Email: madhan.janakiram@manipal.edu.my
Д-р Мадхан Кумар Соуталлу Джанакирам – Ph.D (в области медицины), доц. каф. анатомии, Медицинский факультет, Университетский колледж Манипал, Малайзия.
Email: madhan.janakiram@manipal.edu.my
Dr Arbind Kumar Choudhary – Ph.D (medical), Assistant Professor of Pharmacology Government Erode Medical College and Hospital Erode, India. Email: arbindkch@gmail.com;
ORCID: 0000-0001-8910-1745; Scopus Author ID: 57210737373
Д-р Арбинд Кумар Чоудхари – Ph.D (в области медицины), доц. каф. фармакологии, Государственный медицинский колледж и больница Ироду, Индия. Email: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus Author ID: 57210737373
Received: 26.11.2025
Revised: 22.12.2025
Accepted: 19.02.2026
Поступила в редакцию: 26.11.2025
Поступила после рецензирования: 22.12.2025
Принята к публикации: 19.02.2026
Список исп. литературыСкрыть список1. Mariam Z, Niazi SK. Glucagon-like peptide agonists: A prospective review. Endocrinol Diabetes Metab 2024;7(1):e462. DOI: 10.1002/edm2.462. PMID: 38093651; PMCID:PMC10782143.
2. Olukorode JO, Orimoloye DA, Nwachukwu NO et al. Recent advances and therapeutic benefits of glucagon-like peptide-1 (GLP-1) agonists in the management of type 2 diabetes and associated metabolic disorders. Cureus 2024;16(10):e72080. DOI: 10.7759/cureus.72080. PMID: 39574978; PMCID:PMC11579408.
3. Collins L, Costello RA. Glucagon-Like Peptide-1 Receptor Agonists. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Updated 2024 Feb 29. URL: https://www.ncbi.nlm.nih.gov/books/NBK551568/
4. Myerson M, Paparodis RD. Pharmacotherapy of weight-loss and obesity with a focus on GLP-1 receptor agonists. J Clin Pharmacol 2024;64(10):1204-21. DOI: 10.1002/jcph.2487. PMID: 38924121.
5. Zheng Z, Zong Y, Ma Y et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther 2024;9(1):234. DOI: 10.1038/s41392-024-01931-z. PMID: 39289339; PMCID:PMC11408715.
6. Jones LA, Brierley DI. GLP-1 and the neurobiology of eating control: recent advances. Endocrinology 2025;166(2):bqae167. DOI: 10.1210/endocr/bqae167. PMID: 39813121; PMCID:PMC11745901.
7. Ryan JJ, Marathe CS, Rayner CK et al. Physiology and pharmacology of effects of GLP-1-based therapies on gastric, biliary and intestinal motility. Endocrinology 2025;166(1):bqae155. DOI: 10.1210/endocr/bqae155
8. Liu QK. Mechanisms of action and therapeutic applications of GLP-1 and dual GIP/GLP-1 receptor agonists. Front Endocrinol (Lausanne) 2024;15:1431292. DOI: 10.3389/fendo.2024.1431292. PMID: 39114288; PMCID:PMC11304055.
9. Sztanek F, Tóth LI, Pető A et al. New developments in pharmacological treatment of obesity and type 2 diabetes – beyond and within GLP-1 receptor agonists. Biomedicines 2024;12(6):1320. DOI: 10.3390/biomedicines12061320. PMID: 38927527; PMCID:PMC11201978.
10. Ilias I, Zabuliene L, Rizzo M. GLP-1 receptor agonists in diabetes and weight loss: the double-edged sword of innovation and risks. Front Clin Diabetes Healthc 2025;5:1530811. DOI: 10.3389/fcdhc.2024.1530811. PMID: 39850851; PMCID:PMC11754396.
11. Alfaris N, Waldrop S, Johnson V et al. GLP-1 single, dual, and triple receptor agonists for treating type 2 diabetes and obesity: a narrative review. EClinicalMedicine 2024;75:102782. DOI: 10.1016/j.eclinm.2024.102782. PMID: 39281096; PMCID:PMC11402415.
12. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab 2018;27(4):740-56. DOI: 10.1016/j.cmet.2018.03.001. PMID: 29617641.
13. Moiz A, Filion KB, Tsoukas MA et al. The expanding role of GLP-1 receptor agonists: a narrative review of current evidence and future directions. EClinicalMedicine 2025;86:103363. DOI: 10.1016/j.eclinm.2025.103363. PMID: 40727007; PMCID:PMC12303005.
14. Aoun L, Almardini S, Saliba F et al. GLP-1 receptor agonists: a novel pharmacotherapy for binge eating? A systematic review. J Clin Transl Endocrinol 2024;35:100333. DOI: 10.1016/j.jcte.2024.100333. PMID: 38449772; PMCID:PMC10915596.
15. Cleveland Clinic. GLP-1 agonists. URL: https://my.clevelandclinic.org/health/treatments/13901-glp-1-agonists
16. Endocrinology Advisor. Mechanism of action: GLP-1 agonist. URL: https://www.endocrinologyadvisor.com/features/mechanism-of-action-glp-1-agonist/
17. Ohio State University. Activating GLP-1 naturally. URL: https://health.osu.edu/wellness/exercise-and-nutrition/activiating-glp-1-naturally
18. Chuang MH, Chen JY, Wang HY et al. Clinical outcomes of tirzepatide or GLP-1 receptor agonists in individuals with type 2 diabetes. JAMA Netw Open 2024;7(8):e2427258. DOI: 10.1001/jamanetworkopen.2024.27258. PMID: 39133485; PMCID:PMC11320168.
19. Wen J, Nadora D, Truong A et al. Next-generation dual GLP-1/GIP, GLP-1/glucagon, and triple GLP-1/GIP/glucagon agonists: a literature review. Nutr Metab Cardiovasc Dis 2025 Jun 28:104213. DOI: 10.1016/j.numecd.2025.104213. PMID: 40685266.
20. Kaneko S. Tirzepatide: a novel once-weekly dual GIP/GLP-1 receptor agonist. TouchREV Endocrinol 2022;18(1):10-9. DOI: 10.17925/EE.2022.18.1.10. PMID: 35949358; PMCID:PMC9354517.
21. American College of Cardiology. GLP-1RAs in clinical practice. URL: https://www.acc.org/Latest-in-Cardiology/Articles/2024/04/15/11/19/GLP1RAs-in-Clinical-Practice
22. Karimi MA, Gholami Chahkand MS et al. Comparative effectiveness of semaglutide vs liraglutide, dulaglutide or tirzepatide. Front Pharmacol 2025;16:1438318. DOI: 10.3389/fphar.2025.1438318. PMID: 40444045; PMCID:PMC12120964.
23. Mahase E. GLP-1 agonists linked to adverse gastrointestinal events in weight-loss patients. BMJ 2023;383:2330. DOI: 10.1136/bmj.p2330. PMID: 37813459.
24. Xia L, Li H, Huang S, Shen L. Semaglutide vs dulaglutide for glycemic and weight control. Biomed Rep 2024;22(3):35. DOI: 10.3892/br.2024.1913. PMID: 39781043; PMCID:PMC11704830.
25. Jalleh RJ, Plummer MP, Marathe CS et al. Clinical consequences of delayed gastric emptying with GLP-1 receptor agonists. J Clin Endocrinol Metab 2024;110(1):1-15. DOI: 10.1210/clinem/dgae719. PMID: 39418085; PMCID:PMC11651700.
26. Wong E, Cope R, Dima L, Nguyen T. Tirzepatide for management of type 2 diabetes. Am J Ther 2023;30(1):e26-e35. DOI: 10.1097/MJT.0000000000001588. PMID: 36516422.
27. Aldhaleei WA, Abegaz TM, Bhagavathula AS. GLP-1 receptor agonists associated gastrointestinal adverse events. Pharmaceuticals 2024;17(2):199. DOI: 10.3390/ph17020199. PMID: 38399414; PMCID:PMC10891568.
28. Sklepinski SM, Deng Y, Swarna KS et al. Comparative effectiveness of GLP-1 receptor agonists on cardiovascular outcomes. Diabetes Res Clin Pract 2025;229:112910. DOI: 10.1016/j.diabres.2025.112910. PMID: 40983112.
29. Sokary S, Bawadi H. Promise of tirzepatide: a narrative review. Prim Care Diabetes 2025;19(3):229-37. DOI: 10.1016/j.pcd.2025.03.008. PMID: 40221292.
30. Wen J, How-Volkman C, Truong A et al. Comparative efficacy of semaglutide vs liraglutide or efinopegdutide. Cureus 2024;16(12):e75304. DOI: 10.7759/cureus.75304. PMID: 39776746.
31. Ghusn W, Hurtado MD. GLP-1 receptor agonists for obesity: outcomes and risks. Obes Pillars 2024;12:100127. DOI: 10.1016/j.obpill.2024.100127. PMID: 39286601; PMCID:PMC11404059.
32. Krinsky D, Marcucci A, Mullally JA, Frishman WH. Oral GLP-1 receptor agonists for weight loss. Cardiol Rev. 2024 Dec 17. DOI: 10.1097/CRD.0000000000000833. PMID: 39688941.
33. Gogineni P, Melson E, Papamargaritis D, Davies M. Oral GLP-1 receptor agonists: current status. Expert Opin Pharmacother 2024;25(7):801-18. DOI: 10.1080/14656566.2024.2356254. PMID: 38753454.
34. PR Newswire. Lilly's oral GLP-1 orforglipron superior to oral semaglutide. URL: https://www.prnewswire.com/news-releases/lillys-oral-glp-1-orforglipron-superior-to-oral-semaglutide-in-head-to-head-trial-302559090.html
35. Vergès B, Charbonnel B. Cardiovascular benefits of GLP-1 receptor agonists. Diabetes Metab 2017;43(Suppl 1):2S3-2S12. DOI: 10.1016/S1262-3636(17)30067-8. PMID: 28431669.
36. Jastreboff AM, Kaplan LM, Frías JP et al. Retatrutide for obesity. N Engl J Med 2023;389(6):514-26. DOI: 10.1056/NEJMoa2301972. PMID: 37366315.
37. Andrikou E, Tsioufis C, Andrikou I et al. GLP-1 receptor agonists and cardiovascular outcome trials. Hellenic J Cardiol 2019;60(6):347-51. DOI: 10.1016/j.hjc.2018.11.008. PMID: 30528435.
38. Urva S, Coskun T, Loh MT et al. LY3437943 triple agonist trial. Lancet 2022;400(10366):1869-81. DOI: 10.1016/S0140-6736(22)02033-5. PMID: 36354040.
39. Rosenstock J, Hsia S, Nevarez Ruiz L et al. Orforglipron in early type 2 diabetes. N Engl J Med 2025;393(11):1065-76. DOI: 10.1056/NEJMoa2505669. PMID: 40544435.
40. Zweck E, Roden M. GLP-1 receptor agonists and cardiovascular disease. Lancet Diabetes Endocrinol 2019;7(2):89-90. DOI: 10.1016/S2213-8587(18)30351-6. PMID: 30683221.
41. ClinicalTrials.gov. Study NCT05882045.
42. Karakasis P, Patoulias D, Pamporis K et al. Safety and efficacy of oral GLP-1 agonists orforglipron and danuglipron. Metabolism 2023;149:155710. DOI: 10.1016/j.metabol.2023.155710. PMID: 37852529.
43. Verma S, McGuire DK, Bain SC et al. Liraglutide and semaglutide outcomes across BMI categories. Diabetes Obes Metab 2020;22(12):2487-92. DOI: 10.1111/dom.14160. PMID: 32744418.
44. Sanyal AJ, Kaplan LM, Frias JP et al. Retatrutide for MASLD. Nat Med. 2024;30(7):2037-48. DOI: 10.1038/s41591-024-03018-2. PMID: 38858523.
45. Rivera FB, Cruz LLA, Magalong JV et al. Cardiovascular and renal outcomes of GLP-1 receptor agonists. Am J Prev Cardiol 2024;18:100679. DOI: 10.1016/j.ajpc.2024.100679. PMID: 38779187.
46. ClinicalTrials.gov. Study NCT05931367.
47. Bethel MA, Patel RA, Merrill P et al. Cardiovascular outcomes with GLP-1 receptor agonists. Lancet Diabetes Endocrinol 2018;6(2):105-13. DOI: 10.1016/S2213-8587(17)30412-6. PMID: 29221659.
48. Marathe SJ, Grey EW, Bohm MS et al. Retatrutide and obesity-associated cancer progression. NPJ Metab Health Dis 2025;3(1):10. DOI: 10.1038/s44324-025-00054-5. PMID: 40094000.
49. Siddeeque N, Hussein MH, Abdelmaksoud A et al. Neuroprotective effects of GLP-1R agonists in neurodegenerative disorders. Int Immunopharmacol 2024;143:113537. DOI: 10.1016/j.intimp.2024.113537. PMID: 39486172.
50. Siddeeque N et al. Neuroprotective effects of GLP-1 receptor agonists in neurodegeneration among patients with obesity. Life Sci 2024;359:123133.
51. Lv D, Feng P, Guan X et al. GLP-1 drugs in Parkinson's disease. Front Neurol 2024;15:1462240. DOI: 10.3389/fneur.2024.1462240. PMID: 39719978.
52. Mantovani A, Petracca G, Beatrice G et al. GLP-1 receptor agonists in NAFLD/NASH. Metabolites 2021;11(2):73. DOI: 10.3390/metabo11020073. PMID: 33513761.
53. Hong CT, Chen JH, Hu CJ. GLP-1 receptor agonists in Alzheimer’s and Parkinson’s disease. J Biomed Sci 2024;31(1):102. DOI: 10.1186/s12929-024-01090-x. PMID: 39501255.
54. Nevola R, Epifani R, Imbriani S et al. GLP-1 receptor agonists in NAFLD: evidence and future perspectives. Int J Mol Sci 2023;24(2):1703. DOI: 10.3390/ijms24021703. PMID: 36675217.
55. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in type 2 diabetes: state-of-the-art. Mol Metab 2021;46:101102. DOI: 10.1016/j.molmet.2020.101102. PMID: 33068776.