Клинический разбор в общей медицине №06 2026
Мария Сьюзан Сабу1, Матиха Арикиченане1, Арул Баласубраманиан1, Арбинд Кумар Чоудхари3
1 Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия;
2 Медицинский колледж и больница имени Кирупанандха Варияра миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия;
3 Государственный медицинский колледж и больница Ироду, Ироду, Тамилнад, Индия
kothair@vmpha.edu.in
Аннотация
Введение. Хроническая почечная недостаточность (ХПН) – это серьезное осложнение, развивающееся у пациентов с сахарным диабетом (СД), которое способствует повышению заболеваемости и смертности. Целью исследования было проанализировать частоту и осложнения ХПН у пациентов с СД 2-го типа в специализированной больнице.
Методы. Проспективное наблюдательное исследование проводили на базе специализированной больницы в течение 6 мес (с января по июнь 2024 г.). В исследование включили 100 взрослых пациентов с СД 2-го типа и ХПН, диагностированной в соответствии с рекомендациями KDIGO 2012. Выполнен сбор демографических, клинических и биохимических данных, включая уровень креатинина в сыворотке крови, уровень мочевины в крови, тяжесть альбуминурии.
Результаты. В исследованной популяции 58% были мужчинами, 42% – женщинами, при этом возраст большинства составил 60–69 лет (34%). Выявлен повышенный уровень креатинина в сыворотке (74%) и мочевины в крови (68%), что говорит о значительном нарушении функции почек. Макроальбуминурия (MAA) была наиболее часто встречающейся формой альбуминурии, особенно у пожилых пациентов и некурящих людей. Наиболее частыми сопутствующими заболеваниями были гиперлипидемия (84%), анемия (71%), нарушения зрения (58%), артериальная гипертензия (48%), заболевания щитовидной железы (44%), гиперпродукция соляной кислоты и пепсина (38%), инфекции мочевыводящих путей (34%). Факторы образа жизни, такие как курение и употребление алкоголя, значимо коррелировали с тяжестью альбуминурии.
Выводы. Исследование демонстрирует высокую распространенность ХПН и ее осложнений среди пациентов с СД 2-го типа, особенно среди пожилых мужчин. Регулярный мониторинг функции почек и раннее выявление альбуминурии имеют решающее значение для предотвращения прогрессирования заболевания. Вмешательства, направленные на коррекцию сопутствующих заболеваний и факторов образа жизни, могут улучшить долгосрочные результаты в этой группе высокого риска.
Ключевые слова: хроническая почечная недостаточность, сахарный диабет 2-го типа, макроальбуминурия, креатинин сыворотки крови, мочевина крови, осложнения.
Для цитирования: Котай Рамалингам, Ситараман Ранганатан Рангабасьям, Мадхумитан Раджасельвам, Мария Сьюзан Сабу, Матиха Арикиченане, Арул Баласубраманиан, Арбинд Кумар Чоудхари. Наблюдательное исследование частоты и осложнений хронической почечной недостаточности у пациентов с сахарным диабетом. Клинический разбор в общей медицине. 2025; 7 (6): 29–33. DOI: 10.47407/kr2026.7.6.00859
Introduction
Chronic kidney disease (CKD) and kidney failure are most frequently caused by Diabetes mellitus (DM), an epidemic that is on the rise. Diabetic nephropathy is one of the most prevalent complications associated with diabetes, affecting between 20–40% of people with the disease. The main cause of CKD is diabetes because high blood sugar can harm kidney blood vessel making it more difficult for the kidney to filter waste and extra fluid from the body [1]. DM and CKD have a complicated and reciprocal interaction. Numerous processes, such as oxidative stress, inflammation, and fibrosis brought on by hyperglycaemia, can result in CKD in people with diabetes mellitus [2, 3]. However, by decreasing insulin sensitivity, increasing glucose reabsorption, and encouraging the development of insulin resistance, CKD can worsen DM [4]. Research has repeatedly demonstrated that between 20% and 50% of patients with DM develop CKD. However, the demographic, diagnostic standards, and study design all have a significant impact on the frequency and consequences of CKD in DM patients. Furthermore, CKD is frequently underdiagnosed and undertreated in DM patients, which results in poor health outcomes and higher medical expenses. In addition to ensuring appropriate glycemic control, screening for diabetic nephropathy and early treatments are essential for slowing its progression. Over 10–15% of world population has recognized CKD as a global health issue. Approximately around 422 million adults in the world population are living with DM, 40% of them develop CKD. Diabetic patients with CKD substantially increase the risk of early death and cardiovascular morbidity and mortality.
DM and CKD coexist because they have similar causes, such as aging, vascular inflammation, hypertension, and dyslipidaemia. It is now widely acknowledged that strict glycemic control lowers the risk of retinopathy, neuropathy, and nephropathy in individuals with both type 1 and type 2 diabetes, based on extensive intervention trials. Notably, the probability of negative renal outcomes, such as incident microalbuminuria and progression to macroalbuminuria, is reduced by appropriate glucose control. Trials supporting strict glycemic control as a risk-reduction strategy for individuals with incident cardiovascular disease are scarce, despite the fact that hyperglycaemia is also substantially linked to macrovascular disease in observational trials [5].
The standard measure for renal function and its diagnosis and management is glomerular filtration rate (GFR).According to GFR, the 2012 KDIGO CKD classification divides CKD into 6 groups which includes: G1: GFR 90 mL/min per 1.73 m2 and above, G2: GFR 60 to 89 mL/min per 1.73 m2, G3a: GFR 45 to 59 mL/min per 1.73 m2,G3b: GFR 30 to 44 mL/min per 1.73 m2, G4: GFR 15 to 29 mL/min per 1.73 m2 and G5: GFR less than 15 mL/min per 1.73 m2 or treatment by dialysis [6].
CKD affects more than 10% of the global population over 800 million people and are more common in older adult’s women, racial minorities and those with diabetes or hypertension. It also adds a lot of financial and resource burden on healthcare of any nation [7]. Several CKD registries such as USRDS, provides estimates of the incidence and prevalence of this illness in various countries. Worldwide, DM is the leading cause of CKD an end stage kidney disease accounting for 50% of cases [8].
Progressive CKD is associated with the number of consequences that are more common and severe. These results in increased morbidity and poor quality of life. Hypertension is one of the most harmful complications of CKD and it contributes to the progressive decline in kidney function, cardiovascular disease and related mortality [9]. The risk of cardiovascular events increases with CKD this include non – atherosclerotic pathologies, left ventricular hypertrophy with diastolic and systolic dysfunction, valvular disease and arterial classification. Anaemia is a common complication along with CKD and it can affect the quality of life. It also contributes to the mortality and morbidity of CKD progression rate. CKD patients tend to have inflammatory state; this persistent inflammation can contribute in the variability of HB levels. Iron deficiency anaemia is the most common type of anaemia found in CKD patients. These patients can suffer from both absolute and functional iron deficiency [10]. The association between anaemia and mortality may be related to severity of anaemia. Retinopathy and CKD are typically considered microvascular complications of diabetes. Longer duration of diabetes is one of the main factors along with decreased GFR and more proteinuria contributes to this [11]. Hyperlipidaemia is one of the most prevalent risk factors of CKD, suggesting that lipid accumulation in the renal parenchyma is detrimental to renal function [12]. Mostly CKD patients are at the risk of urinary tract infection, arthritis, acid peptic disease and thyroid disease. There is a lack of regional data on CKD prevalence and complication profiles among diabetic patients in tertiary care hospitals. This study addresses that gap by analysing demographic, biochemical, and lifestyle factors in relation to CKD severity. Therefore, this study was undertaken to assess the prevalence of CKD and its associated complications in patients with T2DM attending a tertiary care hospital. By identifying demographic, clinical, and biochemical correlates, the findings aim to provide insights that could support early intervention strategies and improve patient outcomes. By identifying the associated risk factors and complications, this study seeks to provide insights for developing targeted interventions to mitigate the impact of CKD in diabetic populations.
Materials and methods
A prospective observational study was conducted for 6 months in a tertiary hospital involved 100 patients of both genders having CKD with type 2 DM. The participants were adults (18–80y) with T2DM&CKD (as per KDIGO 2012 classification: GFR <90 mL/min/1.73m2 with evidence of kidney damage) were included. Patients with non-diabetic CKD, pregnancy, incomplete records or kidney transplantation in the previous year were excluded. The study aimed to assess the prevalence of CKD, its associated complications, and the role of various clinical, biochemical, and demographic factors. The proposal of the study was submitted to the institutional review board and received approval (VMKVMC&H/IEC/24/085). Informed consent was obtained from all the patients by the investigators before the patients were involved in the study. The sample size was selected by using non-random purposive sampling technique. A total of 100 patients were selected based on inclusion and exclusion criteria which were regarded as sample size for the study. Data were collected on demographics, clinical characteristics, lifestyle factors, and laboratory parameters, including blood urea, serum creatinine, and albuminuria levels.
Patient inclusion exclusion criteria
Patients who agreed to engage in the study. Patients who have CKD with type 2 DM, who can be both newly discovered or already known case with different socio-economic backgrounds. All the patients were above 18 years and under the age of 80 years. Patients with CKD caused by condition other than diabetes were excluded. Pregnant women and patients with incomplete medical records were excluded. Patients who undergone kidney transplantation within the last year were also excluded.
Data collection
The data collected were the age, gender, BMI, family history of CKD with DM along with smoking status. The data regarding the serum urea, creatinine were used to find the GFR rate. The albuminuria was categorized as microalbuminuria (MA), macroalbuminuria (MAA) and normoalbuminuria (NA) to compare with GFR. The study also listed the complications along with CKD with type 2 DM. Procedures included the collection of cases recording the details from lab reports to the PROFORMA. The glomerular filtration rate along with other complications were monitored. Data were analysed using appropriate statistical methods. Descriptive statistics were used to summarize demographic and clinical characteristics, while comparative analysis was performed to identify correlations between risk factors and disease severity.
 Results
Results
A cross-sectional observational study was conducted among 100 diabetic patients with chronic kidney disease (CKD) at VMKVMC&H, Salem, Tamil Nadu, to investigate the prevalence and complications of CKD in diabetic individuals.
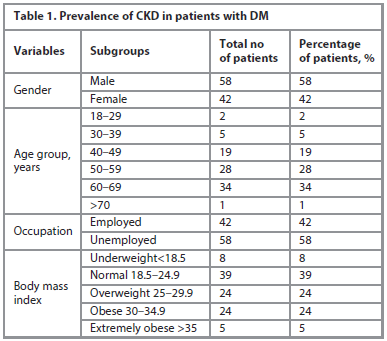
1. Demographic and Clinical Characteristics. The sociodemographic details of the study population was presented in Table 1. It clarifies that out of 100 patients with T2DM and CKD, 58% were male and 42% female, indicating a higher prevalence among males. The largest proportion of patients were in the 60–69 years age group (34%), followed by 50–59 years (28%) and 40–49 years (19%), showing that CKD prevalence increased with age.
Regarding occupation, 58% were unemployed, and 42% employed, reflecting possible socioeconomic influence on disease distribution. In terms of nutritional status, 39% had a normal BMI, while 24% were overweight and 24% obese, suggesting that nearly half of the patients were above normal weight. A smaller proportion were underweighted (8%) or extremely obese (5%).
2. Clinical profile and complications of the study participants. The distribution of variables such as blood pressure, glycemic control, renal parameters, and associated complications was evaluated and presented in Table 2, which highlights the overall burden of metabolic and renal abnormalities as well as the prevalence of comorbid conditions in patients with T2DM and CKD.
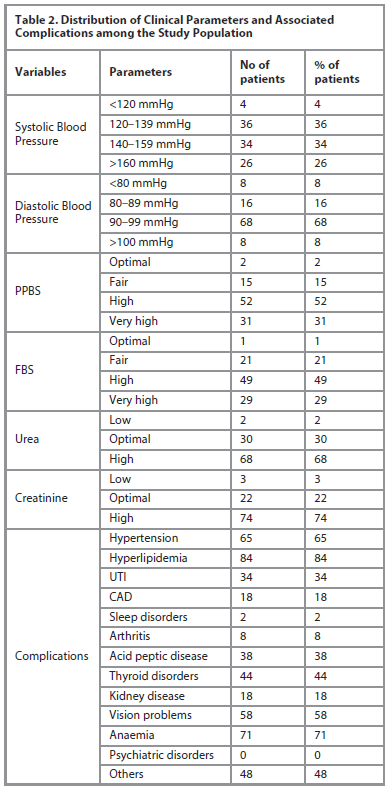 Table 2 elucidates that, among the patients in the study, 4% had systolic blood pressure readings below 120 mmHg, 70% had readings between 120 and 159 mmHg, and 26% had readings above 160 mmHg. Just 24% of diastolic blood pressure readings were below 90 mmHg, whereas the majority (68%) were between 90 and 99 mmHg.
Table 2 elucidates that, among the patients in the study, 4% had systolic blood pressure readings below 120 mmHg, 70% had readings between 120 and 159 mmHg, and 26% had readings above 160 mmHg. Just 24% of diastolic blood pressure readings were below 90 mmHg, whereas the majority (68%) were between 90 and 99 mmHg.
According to glycaemic evaluation, 78% of patients had increased FBS and 83% of patients had high or very high PPBS, whereas only ≤2% of patients had excellent control. Abnormal renal parameters were also common; 68% of patients had increased urea, and 74% had raised creatinine. The most common consequences were hypertension (65%), anaemia (71%), hyperlipidaemia (84%), and visual issues (58%). Urinary tract infections (34%), acid peptic illness (38%), and thyroid disorders (44%), were among the other prevalent ailments. Arthritis (8%), sleep disturbances (2%), and kidney and coronary artery disease (18% each) were fewer common findings. No psychiatric conditions were mentioned.
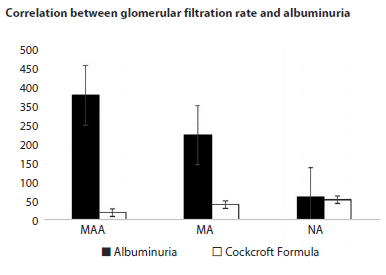
3. Correlation of Albuminuria with Renal Function. On examining the relationship between albuminuria and eGFR, the Figure provides important insights into the pathophysiological link between structural kidney injury and functional impairment, thereby aiding in risk stratification and early intervention strategies.
The relationship between albuminuria levels – categorized as macroalbuminuria (MAA), microalbuminuria (MA), and normal albuminuria (NA) – and estimated glomerular filtration rate (eGFR) calculated using the Cockcroft-Gault formula. Albuminuria values were highest in the MAA group, with significant variability, while eGFR values were consistently lower and demonstrated less intergroup variation.
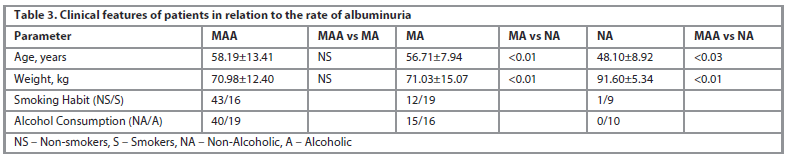
4. Clinical Features and Albuminuria Categories. Comparative evaluation of patients with macroalbuminuria (MAA), microalbuminuria (MA), and normal albuminuria (NA) were demonstrated in Table 3 which provides insights into how age distribution, anthropometric parameters, smoking status, and alcohol consumption are associated with renal impairment.
Table 3 presents the clinical characteristics associated with varying degrees of albuminuria. Patients with MAA and MA were significantly older compared to those with NA (p<0.05). The mean body weight was highest in the NA group (91.6±5.3 kg), whereas patients with MA and MAA had lower mean weights (~71 kg). Interestingly, smoking and alcohol consumption were more common in the NA group, while most MAA patients were non-smokers and non-alcoholic, suggesting complex associations between lifestyle and disease severity.
Discussion
Our study demonstrates a high prevalence of CKD among patients with T2DM, with older age, male gender, and poor glycemic control emerging as major contributors. These findings align with prior Indian studies and reinforce the well-recognized role of diabetes as a leading cause of CKD worldwide. However, the complication profile observed in our cohort, particularly the high rates of hyperlipidaemia and anaemia, suggests a unique pattern that warrants targeted interventions.
Nearly three-quarters of participants exhibited elevated serum creatinine and macroalbuminuria predominated, indicating advanced renal involvement these findings reinforce the well-established role of T2DM as the leading cause of CKD worldwide, accounting for almost 40–50% of ESRD cases. The higher prevalence in males aligns with findings from Bao et al. [13], who reported a gender-related predisposition. Similarly, the predominance of cases in the 60 to 69-year age group is consistent with prior research by Pietro Raven et al. [14], which emphasized age as a critical risk factor.
BMI distribution revealed that patients with normal weight had higher CKD prevalence than overweight or obese groups. While obesity is a well-known risk factor for CKD, this finding suggests that BMI alone may not adequately predict CKD risk in diabetic individuals, pointing to the need for further metabolic profiling.
Family history, smoking, and alcohol use were common in the population. These factors were significantly associated with increased albuminuria and disease progression, as supported by Jan Jeske et al. [15]. Their strong correlation underlines the importance of lifestyle interventions and early education to mitigate risk.
Hypertension, especially systolic readings >140 mmHg and diastolic >90 mmHg, remains a primary driver of diabetic nephropathy. Strict control of glycemic indices, including RBS, FBS, and PPBS, is essential, as glycemic fluctuations contribute to both microvascular and macrovascular damage [16].
Renal function markers such as elevated urea and creatinine levels were present in over two-thirds of patients, reinforcing their value as accessible and sensitive indicators of renal impairment in diabetes.
The complication profile revealed a high incidence of hyperlipidaemia, anaemia, and visual impairment, emphasizing the need for a multidisciplinary approach in diabetes care. The high rate of anaemia is particularly concerning, as it can both result from and exacerbate CKD.
The correlation between albuminuria severity and age, weight, smoking, and alcohol habits suggests that while traditional risk factors contribute significantly, their interplay may be more complex in CKD pathogenesis. Interestingly, the NA group had more smokers and alcohol users, suggesting a need for longitudinal studies to better understand temporal relationships and causality.
Comparison with earlier Indian studies suggests that the prevalence of CKD among people with T2DM is gradually increasing, likely reflecting improved life expectancy, dietary transition, and suboptimal awareness of kidney health.
Conclusion
This study provides valuable insights into the prevalence, risk factors, and complications of chronic kidney disease (CKD) among diabetic patients. The findings underscore the significant burden of CKD in this population, particularly among older adults and males, with notable contributions from lifestyle factors, comorbid conditions, and poor glycemic control. Elevated blood urea and serum creatinine levels were prevalent in most patients, reflecting advanced renal impairment. Albuminuria, a critical diagnostic indicator, showed a higher prevalence of macroalbuminuria (MAA) among older, non-smoking, and non-alcoholic patients. This highlights the need for targeted interventions based on patient-specific risk profiles This study revealed high prevalence of CKD among patients with Type II DM and increased risk of complications such as Hyperlipidaemia, cardiovascular disease and Anaemia. The findings highlight the importance of early screening and management of CKD in patients with DM to prevent or delay the progression of kidney disease and related complications. Regular monitoring of kidney function and implementation of targeted interventions can improve health outcomes and quality of life for this high-risk patient population. Awareness programs and cost-effective screening strategies should be implemented at community and primary care levels. Larger, multicentre, and longitudinal studies are required to confirm these findings and explore genetic or regional variations.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Kothai Ramalingam – Ph.D, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: kothair@vmpha.edu.in; ORCID: 0000-0002-4571-0917; Scopus ID: 10539423000
Котай Рамалингам – Ph.D, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: kothair@vmpha.edu.in; ORCID: 0000-0002-4571-0917; Scopus ID: 10539423000
Sitaraman Ranganathan Rangabasyam – MD, Department of General Medicine, Vinayaka Mission’s Kirupanandha Variyar Medical College & Hospitals, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: rangabashyamsr@yahoo.com; Scopus ID: 57190571666
Ситараман Ранганатан Рангабасьям – д-р медицины, каф. общей врачебной практики, Медицинский колледж и больница имени Кирупанандха Варияра миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: rangabashyamsr@yahoo.com; Scopus ID: 57190571666
Madhumithan Rajaselvam – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: madhumithan263@gmail.com
Мадхумитан Раджасельвам – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: madhumithan263@gmail.com
Mariya Susan Sabu – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: mariyasusansabu@gmail.com
Мария Сьюзан Сабу – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: mariyasusansabu@gmail.com
Matiha Arikichenane – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: mathihamathiha12@gmail.com
Матиха Арикиченане – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: mathihamathiha12@gmail.com
Arul Balasubramanian – Ph. D, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: arul1971@yahoo.com; ORCID: 0000-0001-6896-5069; Scopus ID: 58110901600
Арул Баласубраманиан – Ph.D, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: arul1971@yahoo.com; ORCID: 0000-0001-6896-5069; Scopus ID: 58110901600
Arbind Kumar Choudhary – Ph.D (Medical), Assistant Professor of Pharmacology, Government Erode Medical College and Hospital, Erode, Tamil Nadu 638102, India. E-mail: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus ID: 57210737373
Арбинд Кумар Чоудхари – Ph.D (в области медицины), доц. каф. фармакологии, Государственный медицинский колледж и больница Ироду, Ироду, Тамилнад, Индия. E-mail: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus ID: 57210737373
Received: 02.12.2025
Revised: 29.12.2025
Accepted: 26.02.2026
Поступила в редакцию: 02.12.2025
Поступила после рецензирования: 29.12.2025
Принята к публикации: 26.02.2026
Клинический разбор в общей медицине №06 2026
An observational study on the prevalence and complications of chronic kidney disease in patients with diabetes mellitus
Номера страниц в выпуске:29-33
Abstract
Background. Chronic kidney disease (CKD) is a significant complication in patients with diabetes mellitus (DM), contributing to increased morbidity and mortality. The purpose of the study was to analyse the prevalence and complications of chronic kidney disease in patients with Type II diabetes mellitus in tertiary hospital.
Methods. A prospective observational study was conducted in a tertiary care hospital over six months (January – June 2024). One hundred adult patients with T2DM and CKD, defined according to KDIGO 2012 guidelines, were included. Demographic, clinical, and biochemical data were collected, including serum creatinine, blood urea, and albuminuria. Descriptive and comparative statistical analyses were performed.
Results. Among the study population, 58% were male and 42% female, with the majority aged 60–69 years (34%). Elevated serum creatinine (74%) and blood urea (68%) were observed, indicating significant renal impairment. Macroalbuminuria (MAA) was the predominant category of albuminuria, particularly in older patients and non-smokers. The most frequent comorbidities included hyperlipidaemia (84%), anaemia (71%), vision impairment (58%), hypertension (48%), thyroid disorders (44%), acid peptic disease (38%), and urinary tract infections (34%). Lifestyle factors such as smoking and alcohol consumption were significantly correlated with albuminuria categories.
Conclusion. The study highlights a high prevalence of CKD and its complications among patients with T2DM, particularly in older males. Regular monitoring of renal function and early detection of albuminuria are critical for preventing progression. Targeted interventions addressing comorbidities and lifestyle factors may improve long-term outcomes in this high-risk population.
Keywords: chronic kidney disease, type 2 diabetes mellitus, macroalbuminuria, serum creatinine, blood urea, complications.
For citation: Kothai Ramalingam, Sitaraman Ranganathan Rangabasyam, Madhumithan Rajaselvam, Mariya Susan Sabu, Mathiha Arikichenane, Arul Balasubramanian, Arbind Kumar Choudhary. An observational study on the prevalence and complications of chronic kidney disease in patients with diabetes mellitus. Clinical review for general practice. 2025; 7 (6): 29–33. DOI: 10.47407/kr2026.7.6.00859
Background. Chronic kidney disease (CKD) is a significant complication in patients with diabetes mellitus (DM), contributing to increased morbidity and mortality. The purpose of the study was to analyse the prevalence and complications of chronic kidney disease in patients with Type II diabetes mellitus in tertiary hospital.
Methods. A prospective observational study was conducted in a tertiary care hospital over six months (January – June 2024). One hundred adult patients with T2DM and CKD, defined according to KDIGO 2012 guidelines, were included. Demographic, clinical, and biochemical data were collected, including serum creatinine, blood urea, and albuminuria. Descriptive and comparative statistical analyses were performed.
Results. Among the study population, 58% were male and 42% female, with the majority aged 60–69 years (34%). Elevated serum creatinine (74%) and blood urea (68%) were observed, indicating significant renal impairment. Macroalbuminuria (MAA) was the predominant category of albuminuria, particularly in older patients and non-smokers. The most frequent comorbidities included hyperlipidaemia (84%), anaemia (71%), vision impairment (58%), hypertension (48%), thyroid disorders (44%), acid peptic disease (38%), and urinary tract infections (34%). Lifestyle factors such as smoking and alcohol consumption were significantly correlated with albuminuria categories.
Conclusion. The study highlights a high prevalence of CKD and its complications among patients with T2DM, particularly in older males. Regular monitoring of renal function and early detection of albuminuria are critical for preventing progression. Targeted interventions addressing comorbidities and lifestyle factors may improve long-term outcomes in this high-risk population.
Keywords: chronic kidney disease, type 2 diabetes mellitus, macroalbuminuria, serum creatinine, blood urea, complications.
For citation: Kothai Ramalingam, Sitaraman Ranganathan Rangabasyam, Madhumithan Rajaselvam, Mariya Susan Sabu, Mathiha Arikichenane, Arul Balasubramanian, Arbind Kumar Choudhary. An observational study on the prevalence and complications of chronic kidney disease in patients with diabetes mellitus. Clinical review for general practice. 2025; 7 (6): 29–33. DOI: 10.47407/kr2026.7.6.00859
Наблюдательное исследование частоты и осложнений хронической почечной недостаточности у пациентов с сахарным диабетом
Котай Рамалингам1, Ситараман Ранганатан Рангабасьям2, Мадхумитан Раджасельвам1,Мария Сьюзан Сабу1, Матиха Арикиченане1, Арул Баласубраманиан1, Арбинд Кумар Чоудхари3
1 Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия;
2 Медицинский колледж и больница имени Кирупанандха Варияра миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия;
3 Государственный медицинский колледж и больница Ироду, Ироду, Тамилнад, Индия
kothair@vmpha.edu.in
Аннотация
Введение. Хроническая почечная недостаточность (ХПН) – это серьезное осложнение, развивающееся у пациентов с сахарным диабетом (СД), которое способствует повышению заболеваемости и смертности. Целью исследования было проанализировать частоту и осложнения ХПН у пациентов с СД 2-го типа в специализированной больнице.
Методы. Проспективное наблюдательное исследование проводили на базе специализированной больницы в течение 6 мес (с января по июнь 2024 г.). В исследование включили 100 взрослых пациентов с СД 2-го типа и ХПН, диагностированной в соответствии с рекомендациями KDIGO 2012. Выполнен сбор демографических, клинических и биохимических данных, включая уровень креатинина в сыворотке крови, уровень мочевины в крови, тяжесть альбуминурии.
Результаты. В исследованной популяции 58% были мужчинами, 42% – женщинами, при этом возраст большинства составил 60–69 лет (34%). Выявлен повышенный уровень креатинина в сыворотке (74%) и мочевины в крови (68%), что говорит о значительном нарушении функции почек. Макроальбуминурия (MAA) была наиболее часто встречающейся формой альбуминурии, особенно у пожилых пациентов и некурящих людей. Наиболее частыми сопутствующими заболеваниями были гиперлипидемия (84%), анемия (71%), нарушения зрения (58%), артериальная гипертензия (48%), заболевания щитовидной железы (44%), гиперпродукция соляной кислоты и пепсина (38%), инфекции мочевыводящих путей (34%). Факторы образа жизни, такие как курение и употребление алкоголя, значимо коррелировали с тяжестью альбуминурии.
Выводы. Исследование демонстрирует высокую распространенность ХПН и ее осложнений среди пациентов с СД 2-го типа, особенно среди пожилых мужчин. Регулярный мониторинг функции почек и раннее выявление альбуминурии имеют решающее значение для предотвращения прогрессирования заболевания. Вмешательства, направленные на коррекцию сопутствующих заболеваний и факторов образа жизни, могут улучшить долгосрочные результаты в этой группе высокого риска.
Ключевые слова: хроническая почечная недостаточность, сахарный диабет 2-го типа, макроальбуминурия, креатинин сыворотки крови, мочевина крови, осложнения.
Для цитирования: Котай Рамалингам, Ситараман Ранганатан Рангабасьям, Мадхумитан Раджасельвам, Мария Сьюзан Сабу, Матиха Арикиченане, Арул Баласубраманиан, Арбинд Кумар Чоудхари. Наблюдательное исследование частоты и осложнений хронической почечной недостаточности у пациентов с сахарным диабетом. Клинический разбор в общей медицине. 2025; 7 (6): 29–33. DOI: 10.47407/kr2026.7.6.00859
Introduction
Chronic kidney disease (CKD) and kidney failure are most frequently caused by Diabetes mellitus (DM), an epidemic that is on the rise. Diabetic nephropathy is one of the most prevalent complications associated with diabetes, affecting between 20–40% of people with the disease. The main cause of CKD is diabetes because high blood sugar can harm kidney blood vessel making it more difficult for the kidney to filter waste and extra fluid from the body [1]. DM and CKD have a complicated and reciprocal interaction. Numerous processes, such as oxidative stress, inflammation, and fibrosis brought on by hyperglycaemia, can result in CKD in people with diabetes mellitus [2, 3]. However, by decreasing insulin sensitivity, increasing glucose reabsorption, and encouraging the development of insulin resistance, CKD can worsen DM [4]. Research has repeatedly demonstrated that between 20% and 50% of patients with DM develop CKD. However, the demographic, diagnostic standards, and study design all have a significant impact on the frequency and consequences of CKD in DM patients. Furthermore, CKD is frequently underdiagnosed and undertreated in DM patients, which results in poor health outcomes and higher medical expenses. In addition to ensuring appropriate glycemic control, screening for diabetic nephropathy and early treatments are essential for slowing its progression. Over 10–15% of world population has recognized CKD as a global health issue. Approximately around 422 million adults in the world population are living with DM, 40% of them develop CKD. Diabetic patients with CKD substantially increase the risk of early death and cardiovascular morbidity and mortality.
DM and CKD coexist because they have similar causes, such as aging, vascular inflammation, hypertension, and dyslipidaemia. It is now widely acknowledged that strict glycemic control lowers the risk of retinopathy, neuropathy, and nephropathy in individuals with both type 1 and type 2 diabetes, based on extensive intervention trials. Notably, the probability of negative renal outcomes, such as incident microalbuminuria and progression to macroalbuminuria, is reduced by appropriate glucose control. Trials supporting strict glycemic control as a risk-reduction strategy for individuals with incident cardiovascular disease are scarce, despite the fact that hyperglycaemia is also substantially linked to macrovascular disease in observational trials [5].
The standard measure for renal function and its diagnosis and management is glomerular filtration rate (GFR).According to GFR, the 2012 KDIGO CKD classification divides CKD into 6 groups which includes: G1: GFR 90 mL/min per 1.73 m2 and above, G2: GFR 60 to 89 mL/min per 1.73 m2, G3a: GFR 45 to 59 mL/min per 1.73 m2,G3b: GFR 30 to 44 mL/min per 1.73 m2, G4: GFR 15 to 29 mL/min per 1.73 m2 and G5: GFR less than 15 mL/min per 1.73 m2 or treatment by dialysis [6].
CKD affects more than 10% of the global population over 800 million people and are more common in older adult’s women, racial minorities and those with diabetes or hypertension. It also adds a lot of financial and resource burden on healthcare of any nation [7]. Several CKD registries such as USRDS, provides estimates of the incidence and prevalence of this illness in various countries. Worldwide, DM is the leading cause of CKD an end stage kidney disease accounting for 50% of cases [8].
Progressive CKD is associated with the number of consequences that are more common and severe. These results in increased morbidity and poor quality of life. Hypertension is one of the most harmful complications of CKD and it contributes to the progressive decline in kidney function, cardiovascular disease and related mortality [9]. The risk of cardiovascular events increases with CKD this include non – atherosclerotic pathologies, left ventricular hypertrophy with diastolic and systolic dysfunction, valvular disease and arterial classification. Anaemia is a common complication along with CKD and it can affect the quality of life. It also contributes to the mortality and morbidity of CKD progression rate. CKD patients tend to have inflammatory state; this persistent inflammation can contribute in the variability of HB levels. Iron deficiency anaemia is the most common type of anaemia found in CKD patients. These patients can suffer from both absolute and functional iron deficiency [10]. The association between anaemia and mortality may be related to severity of anaemia. Retinopathy and CKD are typically considered microvascular complications of diabetes. Longer duration of diabetes is one of the main factors along with decreased GFR and more proteinuria contributes to this [11]. Hyperlipidaemia is one of the most prevalent risk factors of CKD, suggesting that lipid accumulation in the renal parenchyma is detrimental to renal function [12]. Mostly CKD patients are at the risk of urinary tract infection, arthritis, acid peptic disease and thyroid disease. There is a lack of regional data on CKD prevalence and complication profiles among diabetic patients in tertiary care hospitals. This study addresses that gap by analysing demographic, biochemical, and lifestyle factors in relation to CKD severity. Therefore, this study was undertaken to assess the prevalence of CKD and its associated complications in patients with T2DM attending a tertiary care hospital. By identifying demographic, clinical, and biochemical correlates, the findings aim to provide insights that could support early intervention strategies and improve patient outcomes. By identifying the associated risk factors and complications, this study seeks to provide insights for developing targeted interventions to mitigate the impact of CKD in diabetic populations.
Materials and methods
A prospective observational study was conducted for 6 months in a tertiary hospital involved 100 patients of both genders having CKD with type 2 DM. The participants were adults (18–80y) with T2DM&CKD (as per KDIGO 2012 classification: GFR <90 mL/min/1.73m2 with evidence of kidney damage) were included. Patients with non-diabetic CKD, pregnancy, incomplete records or kidney transplantation in the previous year were excluded. The study aimed to assess the prevalence of CKD, its associated complications, and the role of various clinical, biochemical, and demographic factors. The proposal of the study was submitted to the institutional review board and received approval (VMKVMC&H/IEC/24/085). Informed consent was obtained from all the patients by the investigators before the patients were involved in the study. The sample size was selected by using non-random purposive sampling technique. A total of 100 patients were selected based on inclusion and exclusion criteria which were regarded as sample size for the study. Data were collected on demographics, clinical characteristics, lifestyle factors, and laboratory parameters, including blood urea, serum creatinine, and albuminuria levels.
Patient inclusion exclusion criteria
Patients who agreed to engage in the study. Patients who have CKD with type 2 DM, who can be both newly discovered or already known case with different socio-economic backgrounds. All the patients were above 18 years and under the age of 80 years. Patients with CKD caused by condition other than diabetes were excluded. Pregnant women and patients with incomplete medical records were excluded. Patients who undergone kidney transplantation within the last year were also excluded.
Data collection
The data collected were the age, gender, BMI, family history of CKD with DM along with smoking status. The data regarding the serum urea, creatinine were used to find the GFR rate. The albuminuria was categorized as microalbuminuria (MA), macroalbuminuria (MAA) and normoalbuminuria (NA) to compare with GFR. The study also listed the complications along with CKD with type 2 DM. Procedures included the collection of cases recording the details from lab reports to the PROFORMA. The glomerular filtration rate along with other complications were monitored. Data were analysed using appropriate statistical methods. Descriptive statistics were used to summarize demographic and clinical characteristics, while comparative analysis was performed to identify correlations between risk factors and disease severity.
ResultsA cross-sectional observational study was conducted among 100 diabetic patients with chronic kidney disease (CKD) at VMKVMC&H, Salem, Tamil Nadu, to investigate the prevalence and complications of CKD in diabetic individuals.
1. Demographic and Clinical Characteristics. The sociodemographic details of the study population was presented in Table 1. It clarifies that out of 100 patients with T2DM and CKD, 58% were male and 42% female, indicating a higher prevalence among males. The largest proportion of patients were in the 60–69 years age group (34%), followed by 50–59 years (28%) and 40–49 years (19%), showing that CKD prevalence increased with age.
Regarding occupation, 58% were unemployed, and 42% employed, reflecting possible socioeconomic influence on disease distribution. In terms of nutritional status, 39% had a normal BMI, while 24% were overweight and 24% obese, suggesting that nearly half of the patients were above normal weight. A smaller proportion were underweighted (8%) or extremely obese (5%).
2. Clinical profile and complications of the study participants. The distribution of variables such as blood pressure, glycemic control, renal parameters, and associated complications was evaluated and presented in Table 2, which highlights the overall burden of metabolic and renal abnormalities as well as the prevalence of comorbid conditions in patients with T2DM and CKD.
Table 2 elucidates that, among the patients in the study, 4% had systolic blood pressure readings below 120 mmHg, 70% had readings between 120 and 159 mmHg, and 26% had readings above 160 mmHg. Just 24% of diastolic blood pressure readings were below 90 mmHg, whereas the majority (68%) were between 90 and 99 mmHg.According to glycaemic evaluation, 78% of patients had increased FBS and 83% of patients had high or very high PPBS, whereas only ≤2% of patients had excellent control. Abnormal renal parameters were also common; 68% of patients had increased urea, and 74% had raised creatinine. The most common consequences were hypertension (65%), anaemia (71%), hyperlipidaemia (84%), and visual issues (58%). Urinary tract infections (34%), acid peptic illness (38%), and thyroid disorders (44%), were among the other prevalent ailments. Arthritis (8%), sleep disturbances (2%), and kidney and coronary artery disease (18% each) were fewer common findings. No psychiatric conditions were mentioned.
3. Correlation of Albuminuria with Renal Function. On examining the relationship between albuminuria and eGFR, the Figure provides important insights into the pathophysiological link between structural kidney injury and functional impairment, thereby aiding in risk stratification and early intervention strategies.
The relationship between albuminuria levels – categorized as macroalbuminuria (MAA), microalbuminuria (MA), and normal albuminuria (NA) – and estimated glomerular filtration rate (eGFR) calculated using the Cockcroft-Gault formula. Albuminuria values were highest in the MAA group, with significant variability, while eGFR values were consistently lower and demonstrated less intergroup variation.
4. Clinical Features and Albuminuria Categories. Comparative evaluation of patients with macroalbuminuria (MAA), microalbuminuria (MA), and normal albuminuria (NA) were demonstrated in Table 3 which provides insights into how age distribution, anthropometric parameters, smoking status, and alcohol consumption are associated with renal impairment.
Table 3 presents the clinical characteristics associated with varying degrees of albuminuria. Patients with MAA and MA were significantly older compared to those with NA (p<0.05). The mean body weight was highest in the NA group (91.6±5.3 kg), whereas patients with MA and MAA had lower mean weights (~71 kg). Interestingly, smoking and alcohol consumption were more common in the NA group, while most MAA patients were non-smokers and non-alcoholic, suggesting complex associations between lifestyle and disease severity.
Discussion
Our study demonstrates a high prevalence of CKD among patients with T2DM, with older age, male gender, and poor glycemic control emerging as major contributors. These findings align with prior Indian studies and reinforce the well-recognized role of diabetes as a leading cause of CKD worldwide. However, the complication profile observed in our cohort, particularly the high rates of hyperlipidaemia and anaemia, suggests a unique pattern that warrants targeted interventions.
Nearly three-quarters of participants exhibited elevated serum creatinine and macroalbuminuria predominated, indicating advanced renal involvement these findings reinforce the well-established role of T2DM as the leading cause of CKD worldwide, accounting for almost 40–50% of ESRD cases. The higher prevalence in males aligns with findings from Bao et al. [13], who reported a gender-related predisposition. Similarly, the predominance of cases in the 60 to 69-year age group is consistent with prior research by Pietro Raven et al. [14], which emphasized age as a critical risk factor.
BMI distribution revealed that patients with normal weight had higher CKD prevalence than overweight or obese groups. While obesity is a well-known risk factor for CKD, this finding suggests that BMI alone may not adequately predict CKD risk in diabetic individuals, pointing to the need for further metabolic profiling.
Family history, smoking, and alcohol use were common in the population. These factors were significantly associated with increased albuminuria and disease progression, as supported by Jan Jeske et al. [15]. Their strong correlation underlines the importance of lifestyle interventions and early education to mitigate risk.
Hypertension, especially systolic readings >140 mmHg and diastolic >90 mmHg, remains a primary driver of diabetic nephropathy. Strict control of glycemic indices, including RBS, FBS, and PPBS, is essential, as glycemic fluctuations contribute to both microvascular and macrovascular damage [16].
Renal function markers such as elevated urea and creatinine levels were present in over two-thirds of patients, reinforcing their value as accessible and sensitive indicators of renal impairment in diabetes.
The complication profile revealed a high incidence of hyperlipidaemia, anaemia, and visual impairment, emphasizing the need for a multidisciplinary approach in diabetes care. The high rate of anaemia is particularly concerning, as it can both result from and exacerbate CKD.
The correlation between albuminuria severity and age, weight, smoking, and alcohol habits suggests that while traditional risk factors contribute significantly, their interplay may be more complex in CKD pathogenesis. Interestingly, the NA group had more smokers and alcohol users, suggesting a need for longitudinal studies to better understand temporal relationships and causality.
Comparison with earlier Indian studies suggests that the prevalence of CKD among people with T2DM is gradually increasing, likely reflecting improved life expectancy, dietary transition, and suboptimal awareness of kidney health.
Conclusion
This study provides valuable insights into the prevalence, risk factors, and complications of chronic kidney disease (CKD) among diabetic patients. The findings underscore the significant burden of CKD in this population, particularly among older adults and males, with notable contributions from lifestyle factors, comorbid conditions, and poor glycemic control. Elevated blood urea and serum creatinine levels were prevalent in most patients, reflecting advanced renal impairment. Albuminuria, a critical diagnostic indicator, showed a higher prevalence of macroalbuminuria (MAA) among older, non-smoking, and non-alcoholic patients. This highlights the need for targeted interventions based on patient-specific risk profiles This study revealed high prevalence of CKD among patients with Type II DM and increased risk of complications such as Hyperlipidaemia, cardiovascular disease and Anaemia. The findings highlight the importance of early screening and management of CKD in patients with DM to prevent or delay the progression of kidney disease and related complications. Regular monitoring of kidney function and implementation of targeted interventions can improve health outcomes and quality of life for this high-risk patient population. Awareness programs and cost-effective screening strategies should be implemented at community and primary care levels. Larger, multicentre, and longitudinal studies are required to confirm these findings and explore genetic or regional variations.
Conflict of interests. The authors declare that there is not conflict of interests.
Конфликт интересов. Авторы заявляют об отсутствии конфликта интересов
Список литературы доступен на сайте журнала https://klin-razbor.ru/
The list of references is available on the journal‘s website https://klin-razbor.ru/
Information about the authors
Информация об авторах
Kothai Ramalingam – Ph.D, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: kothair@vmpha.edu.in; ORCID: 0000-0002-4571-0917; Scopus ID: 10539423000
Котай Рамалингам – Ph.D, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: kothair@vmpha.edu.in; ORCID: 0000-0002-4571-0917; Scopus ID: 10539423000
Sitaraman Ranganathan Rangabasyam – MD, Department of General Medicine, Vinayaka Mission’s Kirupanandha Variyar Medical College & Hospitals, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: rangabashyamsr@yahoo.com; Scopus ID: 57190571666
Ситараман Ранганатан Рангабасьям – д-р медицины, каф. общей врачебной практики, Медицинский колледж и больница имени Кирупанандха Варияра миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: rangabashyamsr@yahoo.com; Scopus ID: 57190571666
Madhumithan Rajaselvam – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: madhumithan263@gmail.com
Мадхумитан Раджасельвам – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: madhumithan263@gmail.com
Mariya Susan Sabu – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: mariyasusansabu@gmail.com
Мария Сьюзан Сабу – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: mariyasusansabu@gmail.com
Matiha Arikichenane – M. Pharma, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: mathihamathiha12@gmail.com
Матиха Арикиченане – магистр фармации, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: mathihamathiha12@gmail.com
Arul Balasubramanian – Ph. D, Department of Pharmacy Practice, Vinayaka Mission’s College of Pharmacy, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: arul1971@yahoo.com; ORCID: 0000-0001-6896-5069; Scopus ID: 58110901600
Арул Баласубраманиан – Ph.D, каф. фармацевтической практики, Фармацевтический колледж миссии Винаяка, Исследовательский фонд миссии Винаяка (признан университетом), Салем, Тамилнад, Индия. E-mail: arul1971@yahoo.com; ORCID: 0000-0001-6896-5069; Scopus ID: 58110901600
Arbind Kumar Choudhary – Ph.D (Medical), Assistant Professor of Pharmacology, Government Erode Medical College and Hospital, Erode, Tamil Nadu 638102, India. E-mail: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus ID: 57210737373
Арбинд Кумар Чоудхари – Ph.D (в области медицины), доц. каф. фармакологии, Государственный медицинский колледж и больница Ироду, Ироду, Тамилнад, Индия. E-mail: arbindkch@gmail.com; ORCID: 0000-0001-8910-1745; Scopus ID: 57210737373
Received: 02.12.2025
Revised: 29.12.2025
Accepted: 26.02.2026
Поступила в редакцию: 02.12.2025
Поступила после рецензирования: 29.12.2025
Принята к публикации: 26.02.2026
Список исп. литературыСкрыть список1. Hahr AJ, Molitch ME. Management of diabetes mellitus in patients with chronic kidney disease. Clin Diabetes Endocrinol 2015 Dec;1(1).
2. Sharma SK, Kant R, Kalra S, Bishnoi R. Prevalence of Primary Non-adherence with Insulin and Barriers to Insulin Initiation in Patients with Type 2 Diabetes Mellitus-An Exploratory Study in a Tertiary Care Teaching Public Hospital. European Endocrinology 2020;16(2):143.
3. Zhuang A, Forbes JM. Stress in the kidney is the road to pERdition: Is endoplasmic reticulum stress a pathogenic mediator of diabetic nephropathy? Journal of Endocrinology 2014;222.
4. Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: Challenges, progress, and possibilities. Clin J American Society of Nephrology 2017;12(12):2032-45.
5. Lubowsky ND, Siegel R, Pittas AG. Management of Glycemia in Patients With Diabetes Mellitus and CKD. Am J Kidney Diseases 2007;50(5):865-79.
6. Teruel JL, Burguera Vion V, Gomis Couto A et al. Elección de tratamiento conservador en la enfermedad renal crónica. Nefrología 2015;35(3):273-9.
7. Ammirati AL. Chronic kidney disease. Revista da Associacao Medica Brasileira 2020;66:3-9.
8. Makmun A, Satirapoj B, Tuyen DG et al. The burden of chronic kidney disease in Asia region: a review of the evidence, current challenges, and future directions. The Korean Society of Nephrology. Kidney Research and Clinical Practice 2025;44:411-33.
9. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med 2015;373(22):210316. DOI: 10.1056/NEJMoa1511939
10. Badve SV, Beller EM, Cass A et al. Interventions for erythropoietin-resistant anaemia in dialysis patients. Cochrane Database of Systematic Reviews. John Wiley and Sons Ltd, 2013.
11. Park YH, Shin JA, Han JH et al. The association between chronic kidney disease and diabetic retinopathy: The Korea National Health and Nutrition Examination Survey. PLoS One 2015;10(4).
12. Suh SH, Kim SW. Dyslipidemia in Patients with Chronic Kidney Disease: An Updated Overview. Korean Diabetes Association. Diabetes and Metabolism Journal 2023;47:612-29.
13. Paneerselvam GS, Kassab YW. Evaluation of glomerular filtration rate estimating equations in ckd patients with diabetes and hypertension. Int J Pharm Pharm Sci 2020;Mar 14:49-52.
14. Stojceva-Taneva O, Otovic NE, Taneva B. Prevalence of diabetes mellitus in patients with chronic kidney disease. Open Access Maced J Med Sci 2016;4(1):79-82.
15. Dunkler D, Kohl M, Heinze G et al. Modifiable lifestyle and social factors affect chronic kidney disease in high-risk individuals with type 2 diabetes mellitus. Kidney Int 2015;87(4):784-91.
16. Muhammad Qamar Rrmisafasnei. Awareness-of-diabetes-mellitus-among-general-public-in-Shah-Alam-Malaysia-A-cross-sectional-study. Asian Journal of Pharmaceutical and Clinical Research 2017;10(Issue 9):193-6.